
New Pediatrics Rotation Exam, Perfect for PA Students
Related Articles



Rosh Review, LLC is not sponsored or endorsed by, or affiliated with, the Physician Assistant Education Association (PAEA) nor the End of Rotation Exam™ (EOR). All trademarks are the property of their respective owners.
The Rotation Exam – Pediatrics, available to Physician Assistant students and programs, is best suited for PA students looking for a focused, high-yield review for the end of your rotation. It joins our growing list of Rotation Exams, including Rotation Exam – Family Medicine, Rotation Exam – Internal Medicine, Rotation Exam – Emergency Medicine, Rotation Exam – Psychiatry and Behavioral Health, and Rotation Exam – Women’s Health. This content is novel and not included in Rosh Review’s PANCE Qbank, Mock exams, or Power Packs.
Topics for the Rosh Review Pediatrics Rotation Exam are based on the national curriculum blueprint.
Categories include the following:
- Dermatology (15%)
- ENOT/Ophthalmology (15%)
- Cardiovascular (10%)
- Pulmonology (12%)
- Gastrointestinal/Nutritional (10%)
- Endocrinology (3%)
- Infectious diseases (12%)
- Psychiatry/behavioral medicine (6%)
- Neurology/developmental (6%)
- Orthopedics/rheumatology (5%)
- Urology/renal (3%)
- Hematology (3%)
Content is organized by task:
- History and Physical (15%)
- Diagnostic studies (10%)
- Diagnosis (25%)
- Health maintenance (10%)
- Clinical intervention (10%)
- Clinical therapeutics (20%)
- Scientific concepts (10%)
Here is an example:
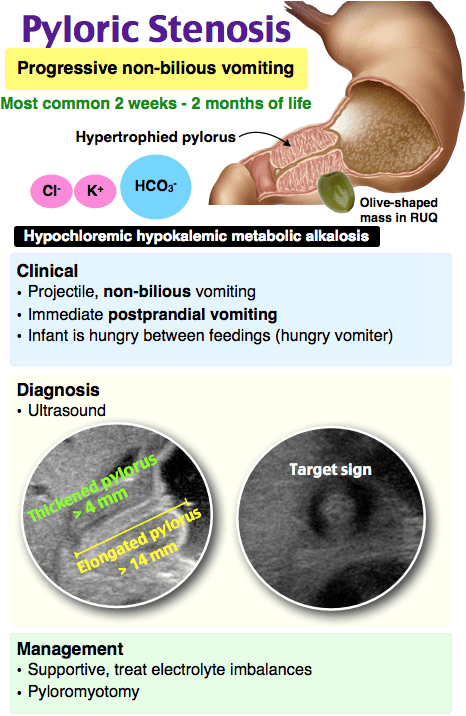
A 5-week-old boy presents with his father to the emergency room because of a 10-day history of vomiting that has become more frequent and more forceful. The vomitus is not bile stained. The infant sucks vigorously and is active, but he is observed to be losing weight. There are no other symptoms noted. Abdominal examination reveals a small, olive-shaped mass upon palpation. Which of the following is the most likely diagnosis?
A. Intussusception
B. Malrotation
C. Pyloric stenosis
D. Volvulus
Answer C
Nonbilious vomiting is the initial symptom of pyloric stenosis. The vomiting may or may not be projectile initially, but is usually progressive, occurring after every feeding. Onset may be as early as the first week of life or as late as five months of age. Diagnosis is established by palpating the pyloric mass, a firm yet movable, 2 cm in length, olive-shaped mass located above and to the right of the umbilicus in the midepigastrium beneath the liver’s edge. Ultrasonography usually confirms the diagnosis, criteria of which includes pyloric thickness of 3–4 mm, overall pyloric length greater than 14 mm and pyloric diameter of 10–14 mm. Contrast studies may also establish the condition, demonstrating an elongated pyloric channel (string sign), a bulge of the pyloric muscle into the antrum (shoulder sign), and parallel streaks of barium seen in the narrowed channel creating a “double tract sign.” Definitive management includes a pyloromyotomy, a traditional Ramstedt procedure done through a short transverse skin incision. Preoperative management includes correction of fluid, acid-base, and electrolyte abnormalities.
Intussusception (A) occurs when a portion of the alimentary tract is telescoped into an adjacent segment. It usually occurs between the ages of 5 months to 3 years. Symptoms include a sudden onset of severe paroxysmal colicky pain recurring at frequent intervals, accompanied by straining efforts with legs and knees flexed and loud cries. Initially comfortable between paroxysms of pain, the infant progressively becomes weaker and lethargic if the intussusception is not reduced. Eventually, a shock-like state with fever and peritonitis can develop. Vomiting is more frequent in the early phase, subsequently becoming bile-stained in the later phase. Infants usually pass a stool containing red blood and mucus, the currant jelly stool. The classic triad of pain, palpable sausage-shaped mass in the abdomen and currant jelly stool is usually seen. Malrotation (B) is characterized by intestinal nonrotation or incomplete rotation around the superior mesenteric artery. It presents in the first year of life with symptoms of acute or chronic obstruction. Infants present in the first week of life with bilious emesis and acute bowel obstruction. In older children, recurrent vomiting and abdominal pain are noted. Symptoms are caused by Ladd bands affecting the small and large bowel. Volvulus (D) is a life-threatening complication of malrotation. It occurs when the small bowel twists around the superior mesenteric artery leading to vascular compromise of the bowel. It may manifest as an acute presentation of small bowel obstruction with bilious emesis, hemodynamic instability, abdominal distention, abdominal tenderness, peritonitis, and hematochezia.
One Step Further question:
Persistent vomiting in a patient with pyloric stenosis can cause mild to moderate dehydration, leading to what type of electrolyte/metabolic disturbance?
Answer:
Hypochloremic, hypokalemic metabolic alkalosis.
Since these categories and tasks are integrated into our improved performance and feedback page, you have access to robust data to help you fine-tune your studying.
Study on…
The Rosh Review Team
A bolus of confidence. A lifetime of knowledge.

Comments (0)