
Podcast Ep 22: Pneumothorax, Vaginal Bleeding, & More



No matter what people tell you, words and ideas can change the world.
-Robin Williams
Welcome back to Episode 22! This week, we have some bread-and-butter emergency medicine with a lot of deeper learning points, so pay close attention as you listen through. Let’s start out with a review of pediatrics before we jump into the new material.

- In treating epiglottitis, the first priority is airway management. Once the airway has been secured, it can be treated with either ampicillin-sulbactam or ceftriaxone.
- The five congenital cyanotic heart defects can be remembered with the numbers 1 to 5.
- One for trucus arteriosus in which the two vessels join to make one.
- Two for transposition of the great vessels in which the two great vessels are switched.
- Three for tricuspid atresia, remember three for tricuspid.
- Four for the four defects of tetralogy of Fallot.
- Five for the five words in total anomalous pulmonary vascular return.
- The three common acyanotic heart lesions are atrial septal defects, ventricular septal defects, and patent ductus arteriosus
Now onto this week’s podcast
Question 1

A 19-year-old woman presents with acute onset of shortness of breath and chest pain. The patient’s chest X-ray is shown above. Which of the following provides definitive management for the condition?
A. Chest thoracostomy tube
B. Intubation and mechanical ventilation
C. Needle decompression
D. Percutaneous pigtail catheter placement
Question 2
A 25-year-old 36-week pregnant woman presents to the ED with a complaint of vaginal bleeding. She denies associated cramping, abdominal pain, or preceding traumatic event. She describes the blood as “bright red.” Which of the following is a risk factor for the development of this condition?
A. Previous caesarean section
B. Previous ectopic pregnancy
C. Primiparity
D. Young maternal age
Question 3
An 18-year-old man presents with an injury to his left index finger. The patient was cleaning the nozzle of a high-pressure paint injector when it fired and punctured his finger. The patient reports pain at the site. On exam, you note a small puncture wound and no exit wound. There is no erythema and the site is mildly tender to palpation. Plain films do not demonstrate a fracture. Which of the following is the most appropriate next step in management?
A. Consult a hand surgeon
B. Perform a digital block for wound exploration
C. Perform high-pressure syringe irrigation
D. Place a sugar-tong splint for immobilization
Question 4
A scuba diver returns to the surface and is unconscious. Which of the following is the likely diagnosis?
A. Air embolism
B. Bends
C. Cerebral edema
D. Nitrogen narcosis
Question 5

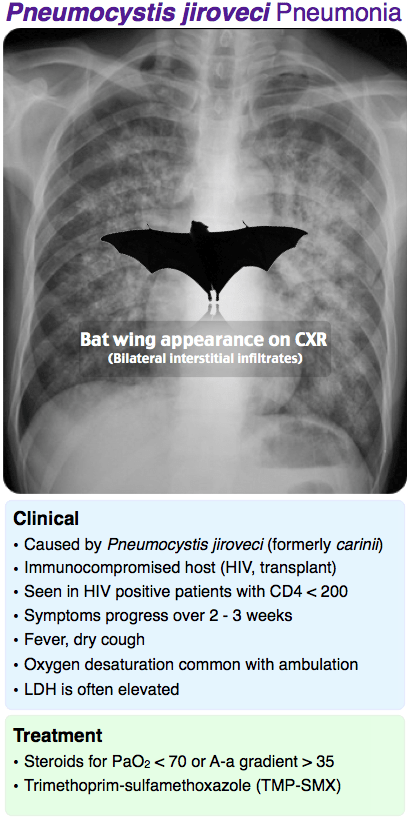
A 34-year-old woman with HIV presents with a cough and shortness of breath. Her oxygen saturation is 93% on room air, partial arterial oxygen tension of 75 mm Hg, and A-a gradient of 30 mm Hg. Her chest X-ray is shown above. What treatment is indicated?
A. Azithromycin and outpatient follow-up
B. Bronchodilators and corticosteroids
C. Doxycycline
D. Trimethoprim-sulfamethoxazole (TMP-SMX)
Question 6
A 16-year-old girl presents with pain to the right index finger after slamming it in a car door. Physical examination reveals a 50% subungual hematoma, and an X-ray shows a nondisplaced distal tuft fracture. What management is indicated?
A. Oral antibiotics, splinting, and follow-up
B. Splinting and follow-up
C. Trephination, splinting, and follow-up
D. Trephination, splinting, oral antibiotics, and follow-up
- A tension pneumothorax may be managed immediately with needle decompression. Definitive management is with chest tube placement.
- In patients with a pneumothorax more than a few days old, rapid re-expansion of the lung can lead to re-expansion pulmonary edema.
- Placenta previa is caused by placental implantation in the lower uterine segment, either completely or partially overlying the cervical OS.
- Placenta previa typically causes painless, bright red vaginal bleeding in the 2nd or 3rd trimester. The abdominal exam will be benign.
- Risk factors for placenta previa include prior caesarean section, advanced maternal age, grand multiparity, previous placenta previa, multiple gestations, previous multiple induced abortions, and preterm labor.
- High-pressure injection injuries should be treated with broad-spectrum antibiotics, extremity elevation, and hand surgery consultation. They carry significant morbidity with delayed treatment leading to tissue necrosis, infection, and possible amputation.
- Suspect an air embolism whenever any diver loses consciousness upon ascent or within 10 minutes of surfacing.
- Air embolisms can cause a wide range of symptoms, including stroke-like symptoms, dyspnea, hemoptysis, chest pain, and dysrhythmias. They are treated with hyperbaric recompression.
- Nitrogen narcosis occurs in dives beyond 100 feet due to an increased concentration of dissolved nitrogen. Symptoms including impaired motor function and behavior problems.
- The bends is a dysbarism that occurs due to rapid ascent. It presents with diffuse muscle and joint pain due to nitrogen bubble release into the tissues.
- PJP Pneumonia is associated with diffuse interstitial infiltrates, classically in a bat wing appearance. It is treated with trimethoprim-sulfamethoxazole. If the arterial oxygen tension is less than 70 or the a-a gradient is greater than 35, corticosteroids have been shown to reduce mortality.
- Histoplasmosis is found in the Ohio and Mississippi river valleys and is associated with bird and bat droppings.
- Blastomycosis is found in the southeast US. In addition to pneumonia, it can cause bone lesions.
- Coccidioidomycosis is found in the southwest US. It is associated with erythema nodosum and arthritis.
- Legionella pneumonia is associated with hyponatremia and gastrointestinal symptoms.
- Distal tuft fractures are treated with nail trephination (if indicated), splinting, and follow up.
- Nail trephination can be accomplished with a heated 18-gauge needle or paperclip, or with an electrical cautery device. A single hole usually adequately relieves the pressure with the evacuation of a drop or two of blood.
That wraps up Episode 22. Remember to follow us on Twitter @Roshcast for updates and high yield EM pearls in 140 characters or less. Curious about the data driving Rosh Review? Check out Sean Michael’s post to get an inside look at the data and the educational philosophy at Rosh Review. Hope to see some of you at CORD!
Until next time,
Jeff and Nachi

{kind=link}
{kind=link}
Comments (0)