
Ambulatory Family Medicine Module For the ABFM Cert Exam Is Now Ready
Related Articles



Announcing the release of a new ABFM Ambulatory Family Medicine Content-Specific Module, available to Family Medicine residents, residency programs, and practicing physicians. This module is best suited for Family Medicine physicians looking for a focused, high-yield Qbank review for ABFMs Content-Specific Modules required during the certification exam. This content is novel, and not included in Rosh Review’s main Family Medicine Qbank or mock exams.
Family Medicine programs that subscribe to Rosh Review also gain access to the Content-Specific Modules in their PD Dash.
Categories include:
- Common office emergencies
- Minor trauma
- Acute diseases
- Chronic diseases
- Preventive care
- Psychosocial and behavioral issues
- Test characteristics
Content is organized by task:
- History and Physical
- Diagnostic studies
- Diagnosis
- Health maintenance
- Clinical intervention
- Clinical therapeutics
- Scientific concepts
Here is an example:
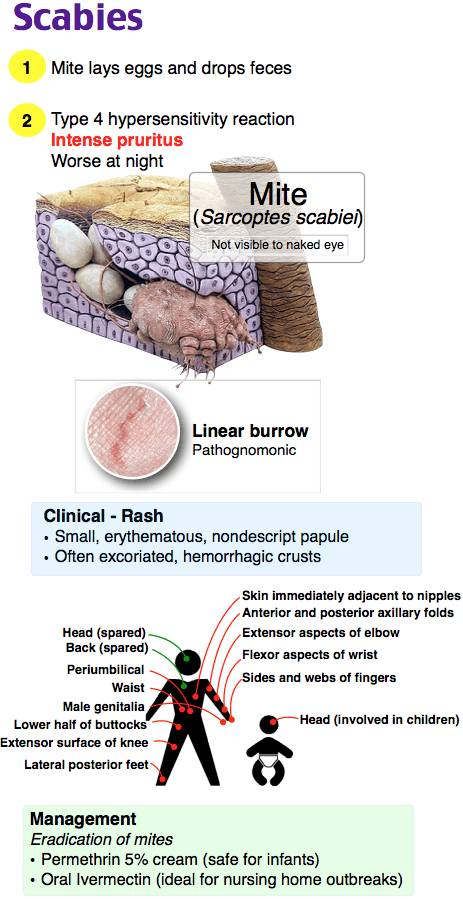
A 56-year-old man presents with an intensely pruritic generalized rash that is worse at night. On examination, you detect excoriations and short, wavy, scaly lines in the finger web spaces and on the wrists. Examination of skin scrapings under the microscope reveals scabies mites. What is first-line treatment for this condition?
A. Benzyl alcohol 5% lotion on day one, then reapply in one week
B. Ivermectin 200 mcg/kg orally on day one, then repeat in one week
C. Permethrin 5% cream on day one, then reapply in one week
D. Spinosad 0.9% suspension on day one, then reapply in one week
Answer C
Permethrin 5% cream on day one, then reapply in one week is considered first-line treatment for scabies. Scabies is more common in young children. Risk factors include overcrowding, poor hygiene, homelessness, dementia, and sexual contact. Transmission occurs via direct skin contact for a duration of 15 to 20 minutes. Diagnosis can be made with a history of pruritus, characteristic distribution of lesions, and itching in close contacts. Pruritic papules, pustules, vesicles, and nodules are the primary skin lesions. The pathognomonic finding is a burrow. An oil scraping of a non-excoriated burrow or papule may reveal mites, eggs, or fecal pellets under the microscope. Treatment is with permethrin 5% cream applied from the neck down for eight to 14 hours, washed off, and then reapplied in one week. Oral ivermectin is also an option. Itching may continue for two weeks afterwards. Sheets and clothing should be washed at 140°F and dried in a hot dryer. The items can also be isolated in a plastic bag for 72 hours.
The CDC also considers a single dose of oral ivermectin (B) at 200 mcg/kg repeated at day 14 (not day seven) as a first-line treatment option for scabies. Its use is limited by cost. Benzyl alcohol 5% lotion (A) and spinosad 0.9% suspension (D) are pharmacologic treatments for head lice.
One Step Further question:
In which type of scabies is pruritus often mild or absent?
Answer:
Crusted or Norwegian scabies.
Since these categories and tasks are integrated into our improved performance and feedback page, you have access to robust data to help you fine-tune your studying and resources to help increase your Family Medicine Certification Exam score by 100 points.
Or visit the main Family Medicine Qbank page to learn about our ABFM Certification Qbank.
Study on…
The Rosh Review Team
A bolus of confidence. A lifetime of knowledge.

Comments (0)