
NEW NCCPA Content Blueprint and Task Area Guidelines Released for 2019

Related Articles



The NCCPA released their updated Content Blueprint guidelines for the 2019 PANCE. Many of the organ systems were updated along with the task areas. In addition to changes in the core content topics, 5% (from 2%) of the PANCE will now cover Professional Practice (formerly legal and ethical questions) issues.
We analyzed the new guidelines for 2019 and made the following comparison
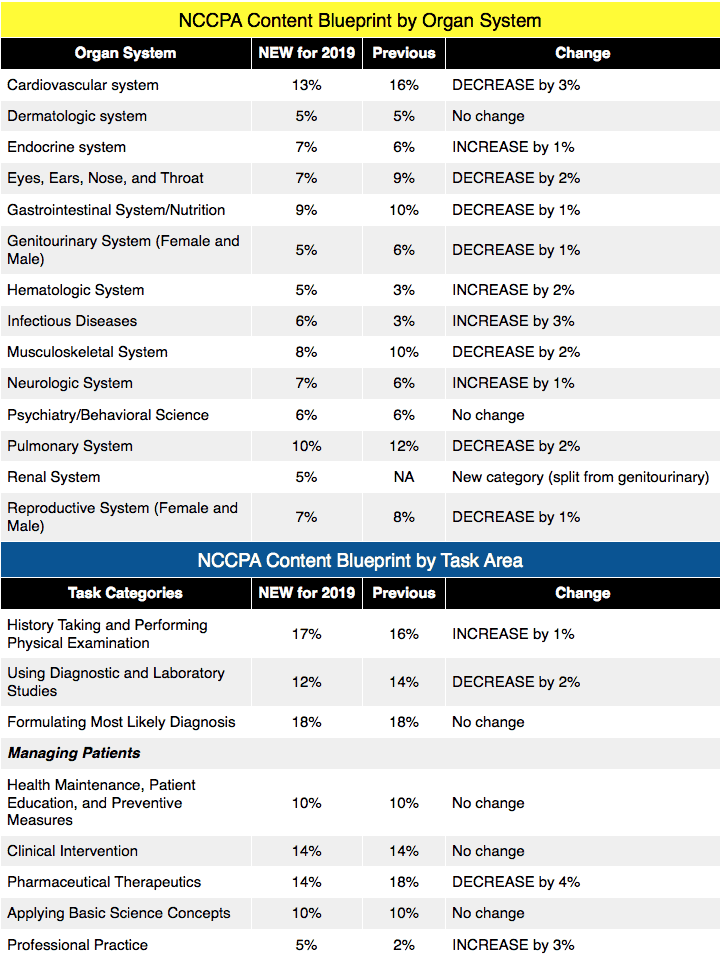
Our analysis came from information published by the NCCPA. Here is the most updated version of the PANCE Content Blueprint released by the NCCPA.
This is the current version, which will be replaced by the new 2019 content blueprint.
Rosh Review is already prepared to make the necessary updates to our content to reflect the changes released by the NCCPA. Rosh Review will modify our categories and subcategories and task areas to reflect the new 2019 NCCPA Content Blueprint categories and task areas. In addition, we are adding more content in Professional Practice to reflect the 3% increase in content in the 2019 NCCPA Content Blueprint.
Rosh Review continues to be the best Qbank for PANCE Board Review.
See for yourself by signing up for a free trial. No risk, all value.
Here is a sneak peak
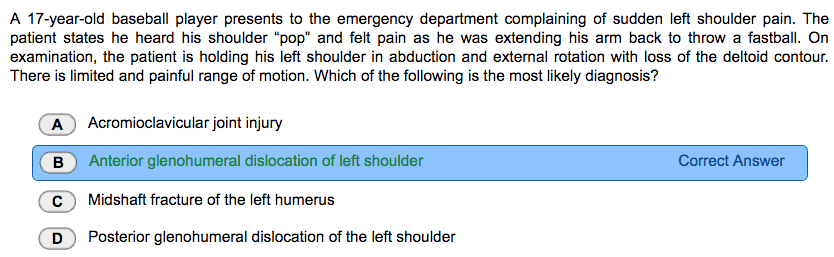
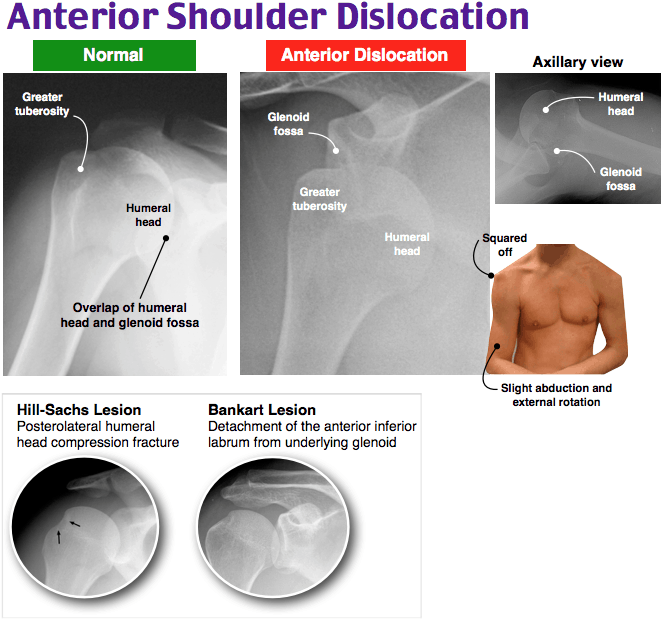
The patient suffered an anterior glenohumeral dislocation of his left shoulder. The shoulder is the most commonly dislocated joint in the body. Dislocations can occur from a trauma (95%) or from laxity of the ligaments (5%). The glenohumeral ligaments, the rotator cuff muscles, and the joint capsule or labrum stabilizes the shoulder. The shoulder joint is often injured during a fall on an outstretched arm, engaging in sports activities, a direct blow to the joint, or grand mal seizures. Patients often report hearing or feeling a pop during the incident and present with significant pain, limited range of motion, swelling, or deformity. Anterior shoulder dislocations are the most common type; however, they can occur posteriorly and inferiorly. Anterior dislocations result from a force applied to the shoulder while the arm is abducted and externally rotated such as while throwing a ball. On examination, the arm is held in abduction and external rotation (down adjacent to the body) with a loss of the deltoid contour when compared to the other shoulder, and the humeral head can often be palpated anteriorly beneath the clavicle. The patient will have very limited range of motion and be unable to touch the opposite shoulder. Obtaining pre-reduction and post-reduction radiographs and neurovascular examinations are imperative to successful management. Complications of shoulder dislocations include fractures (e.g. Hill-Sachs lesion), soft tissue injury (e.g. Bankart lesion), nerve injury (e.g. axillary nerve), or vascular injury (e.g. axillary artery).
Posterior glenohumeral dislocations (D) are much more uncommon and are typically a result from significant adduction and internal rotation caused by a fall on an outstretched arm, a seizure, or a direct blow to the anterior shoulder. The shoulder will be held in adduction and internal rotation (across the chest), the anterior shoulder will appear square with a flat coracoid process, and the humeral head may be palpated posteriorly beneath the acromion process. Bilateral dislocations are rare and are most often a result of a seizure, but shoulders can appear identical leading to a missed diagnosis. Individuals will be unable to abduct or externally rotate the shoulder with a posterior dislocation. A midshaft fracture of the humerus (C) is often caused by a fall on an outstretched arm or a direct blow. However, the fracture may be due to pathological process especially in young children. Upper arm pain, swelling, deformity, limb shortening, and crepitus on palpation are classic presenting symptoms of this type of injury. Appropriate imaging and neurovascular examination is important to determining the severity of the fracture and ultimate management. These fractures are classically associated with wrist drop due to radial nerve injury. An acromioclavicular joint injury (A) also results from trauma and is the second most common shoulder injury in athletes. The acromioclavicular joint consists of 2 bones, the clavicle and acromion, connected by ligaments (acromioclavicular ligament and coracoclavicular ligament) and a meniscal disc. The mechanism of action is commonly due to indirect force on the joint from a fall onto the shoulder with the arm in an adducted position, a downward force onto the shoulder, or a fall on an outstretched hand. The injury occurs because the clavicle maintains its anatomical position while the acromion is forced in a downward direction injuring the ligaments or causing a fracture. There are varying severity of acromioclavicular separation depending on damage to the ligaments. Patients present with superior shoulder pain often with point tenderness over the acromioclavicular joint, swelling, bruising, and pain at night when lying on the involved shoulder. Range of motion will also be reduced specifically when asked to raise the arm.
Rotation Exams
As a subscriber to Rosh Review, you’ll have exclusive access to purchase our Rotation Exams for Emergency Medicine, Internal Medicine, Family Medicine, General Surgery, Psychiatry and Behavioral Health, Women’s Health, and Pediatrics.
Let us know what you think.

Comments (0)