Correct Answer
Distractors
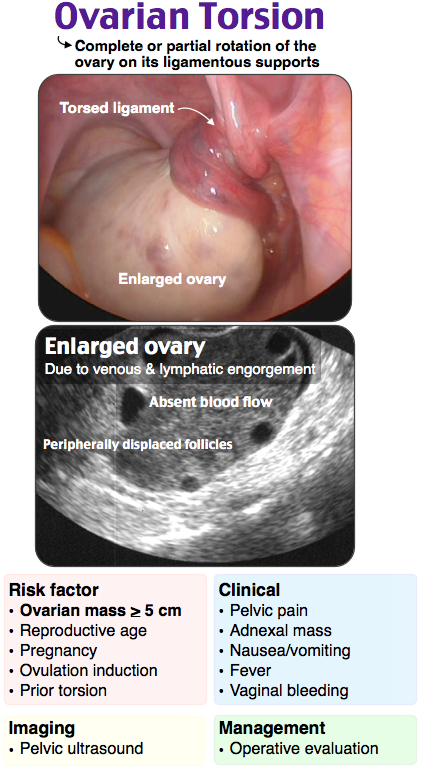
Ovarian torsion is a surgical emergency that requires prompt diagnosis and treatment to preserve ovarian function. It results in an ischemic condition that is almost always associated with ovarian enlargement, usually due to ovarian cysts or masses. This enlargement causes the ovary to twist, resulting in blockage of venous return and arterial occlusion. However, in some cases, only venous return will be blocked, or only one of the two arterial supplies will be occluded. Also, in some cases, the ovary has been known to twist and untwist. Thus, Doppler ultrasound may appear normal in some cases, and thus a high index of suspicion is required when approaching these patients to avoid delayed diagnosis. Classically, the clinical features include unilateral lower abdominal pain and guarding, unilateral adnexal tenderness on bimanual exam, and the presence of a latero-uterine mass. The diagnosis is often made with Doppler of the ovary, but definitive diagnosis is enabled via direct visualization with laparoscopy. An ovary measuring > 4 cm due to cyst, tumor, or edema is the most common ultrasonographic finding associated with torsion, and its presence, even with a normal Doppler study, should be worrisome for torsion. Other findings on ultrasound that are concerning for ovarian torsion include peripherally displaced follicles due to edema of the ovary and a positive whirlpool sign, representing twisting of the vascular pedicle. Treatment is surgical correction, so close consultation with OB/GYN is critical, even in suspected cases with normal Doppler results.
Ovarian torsion is a surgical emergency that requires prompt diagnosis and treatment to preserve ovarian function. It results in an ischemic condition that is almost always associated with ovarian enlargement, usually due to ovarian cysts or masses. This enlargement causes the ovary to twist, resulting in blockage of venous return and arterial occlusion. However, in some cases, only venous return will be blocked, or only one of the two arterial supplies will be occluded.… Read More
Appendicitis (A) occurs when luminal obstruction of the vermiform appendix occurs, typically secondary to a fecalith. Patients classically present with pain in the RLQ over McBurney point. Guarding, abdominal rigidity, and rebound tenderness are usually present. Although appendicitis should be within the differential for the patient above, her pain is mostly located in the pelvis and she has ultrasound findings consistent with ovarian torsion. A hemorrhagic ovarian cyst (B) is a common cause of pelvic pain and occurs when a blood vessel inside the cyst wall ruptures. Patients present with pelvic pain, often acute in onset, and will have findings on ultrasound of an ovarian cyst and free fluid in the pelvis. Tubo-ovarian abscesses (D) are most commonly a late complication of pelvic inflammatory disease, and the majority have associated peritonitis, fever, vaginal discharge, and cervical motion tenderness.