
Podcast Ep 25: Acute Mountain Sickness, Hyperthyroidism, & More



No act of kindness, no matter how small, is ever waster.
-Aesop
Welcome back to Episode 25—our silver anniversary episode! It was great connecting with a few listeners recently at SAEM. At the beginning of this week’s episode, we announced a new contest – be the first to tweet to us (@Roshcast) or email (Roshcast@roshreview.com) the exact time in episodes 26-30 that you hear a trauma phone ring tone to win a 30-day subscription to Rosh Review! First, let us get started with a rapid review covering fish poisonings.

- Hot and cold sensation reversal is classically associated with ciguatera poisoning.
- In scombroid poisonings, patients have reported a metallic, bitter, or even peppery taste.
- In scombroid poisonings, histidine is broken down into histamine. Treat patients supportively with antihistamines.
Now onto this week’s podcast
Question 1
You are on a 10-day mountain climbing excursion in Colorado with one of your 55-year-old coworkers. After ascending to an altitude of 9200 feet, your coworker develops a mild bifrontal headache associated with nausea. He reports feeling “hung over” but denies drinking any alcohol the previous night. He has no other symptoms. On examination, there are no focal neurologic deficits. He desires to continue the climb. Which of the following is the most appropriate next step in the management of your coworker?
A. Administer acetazolamide
B. Administer dexamethasone
C. Arrange to be airlifted to a lower altitude
D. Continue to ascend but at a slower rate
Question 2
A 27-year-old woman, G2P1, presents with vaginal bleeding and right lower quadrant pain. She reports a positive pregnancy test and LMP 6 weeks prior to her evaluation. Vital signs are T 98.6°F, BP 110/68, HR 72, and RR 16. Her abdomen is soft with mild tenderness in the right pelvic area. Pelvic examination is notable for a small amount of red blood in the vagina and mild right adnexal tenderness. Bedside ultrasound shows an empty uterus and adjacent to the right ovary a gestational sac with yolk sac and fetal pole. Which of the following is a contraindication to methotrexate administration?
A. Fetal heart activity
B. Gestational sac greater than 2.5 cm in diameter
C. hCG level of 3000
D. History of ectopic pregnancy
Question 3
A 32-year-old woman, G2P1, at 33 weeks gestation presents to the emergency room for sharp abdominal pain. She has not had any prenatal care during this pregnancy. Her symptoms include vaginal bleeding, uterine pain between contractions, and fetal distress. Her first pregnancy was uncomplicated, with a vaginal delivery at term. Which one of the following is the most likely diagnosis?
A. Placenta previa
B. Placental abruption
C. Uterine rupture
D. Vasa previa
Question 4
Perforation of which gastrointestinal structure is associated with the highest mortality?
A. Cecum
B. Duodenum
C. Esophagus
D. Stomach
Question 5
An 18-year-old woman presents with fever, confusion, weight loss, and palpitations. Her vital signs are T 100.7°F, HR 140, BP 143/93, RR 20, oxygen saturation 95%, and finger stick glucose of 118. Physical examination reveals a thin woman who is alert and oriented x3 with a regular, fast heart rate, and brisk reflexes. Her roommate tells you that the patient has been taking a friend’s levothyroxine in an attempt to lose weight. What management should be initiated?
A. Beta-blocker
B. Beta-blocker, dexamethasone
C. Beta-blocker, dexamethasone, propylthiouracil, and potassium iodide
D. Calcium channel blocker, dexamethasone
Question 6

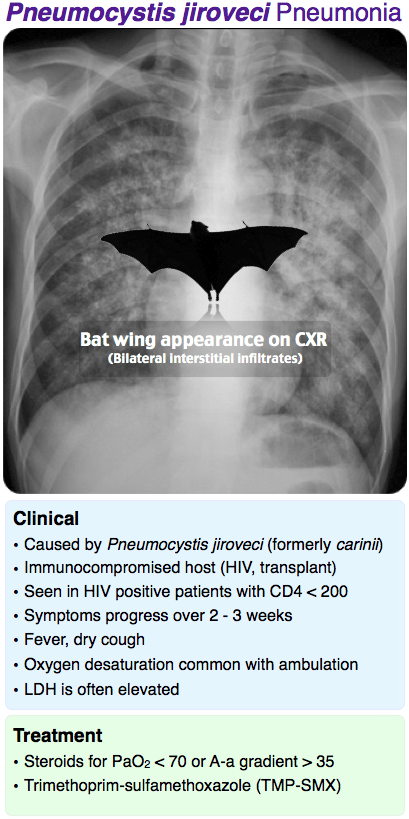
A 53-year-old man complains of fever and non-productive cough. He is also short of breath with exertion. His X-ray is shown above. Which test will be an important part of his overall evaluation?
A. HIV antibody
B. Purified protein derivative skin test
C. Urine Histoplasma antigen
D. Urine Legionella antigen
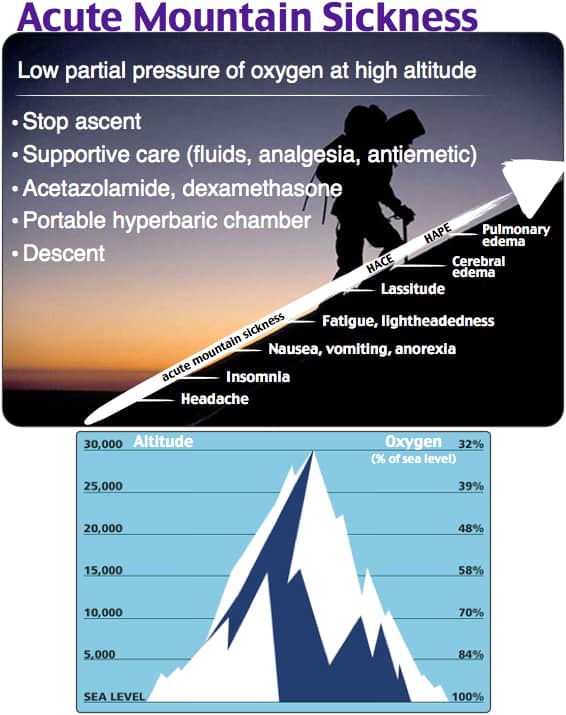
- Acute mountain sickness is characterized by headache, nausea, dizziness, and sleep disturbances after rapid ascent of an unacclimatized person at 2000 meters or higher.
- Mild acute mountain sickness should be treated first by halting ascent and then supportively with fluids, oxygen, analgesia, and anti-emetics. Acetazolamide and dexamethasone can be used as a second-line agent.
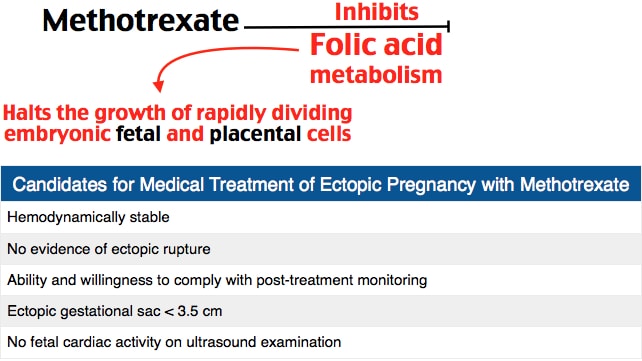
- When medically managing an ectopic pregnancy, methotrexate is relatively contraindicated when fetal heart activity is present, and contraindicated with hemodynamic instability or evidence of rupture on ultrasound. To be eligible for the treatment you need to have a gestational sac less than 3.5 cm and be able and willing to comply with post-treatment monitoring.
- Risk factors for an ectopic pregnancy include prior ectopic pregnancies, history of PID, tubal surgery, or an IUD.
- The fallopian tube is the most common location of an ectopic pregnancy.
- Interstitial ectopic pregnancies occur with implantation of the developing fetus in the interstitium of the myometrium. In such cases, the sac may have an eccentric appearance on sonography, but there would be a thin endomyometrial mantle.
- Placental abruption typically manifests as painful vaginal bleeding with evidence of fetal distress in the third trimester. Often the fundus will be tender and the patient will likely have pain between contractions.
- Common risk factors for placental abruption include abdominal trauma, maternal hypertension, smoking, cocaine use, multiple gestation, and previous abruption.
- Uterine rupture classically presents with a sudden tearing uterine pain with contractions with pain free intervals between contractions.
- Placenta previa usually manifests as painless vaginal bleeding in the late 2nd or 3rd trimesters due to placental tissue overlying the internal cervical os.
- Vasa previa occurs when the umbilical cord inserts into the membranes of the lower uterine segment and amniotic blood vessels present in front of the fetal head. This usually presents with hemorrhage after amniotomy or spontaneous rupture of membranes.
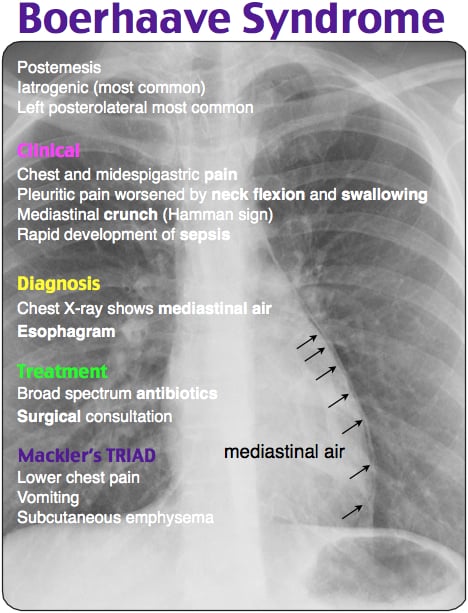
- Esophageal rupture carries significant morbidity and mortality. It should be treated with immediate antibiotics and a surgical consultation.
- More than 90% of spontaneous esophageal ruptures occur in the distal esophagus.
- With blunt trauma to the neck or thorax, esophageal rupture is usually in the proximal or middle third of the esophagus. Iatrogenic injuries frequently occur at the pharyngoesophageal junction.
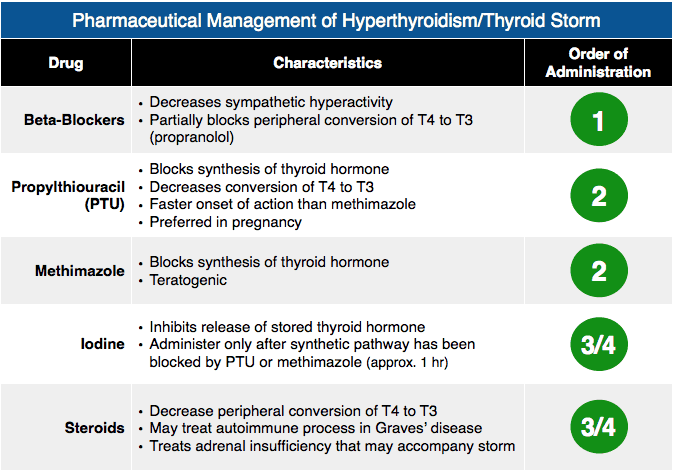
- Endogenous thyroid storm is treated with beta-blockers, PTU, potassium iodide, and dexamethasone. Exogenous thyroid storm is treated with beta-blockers and dexamethasone.
- In thyroid storm, propranolol reduces peripheral conversion of T4 to T3. PTU blocks synthesis of thyroid hormone.
- Potassium iodide blocks the release of thyroid hormone. Dexamethasone blocks the peripheral conversion of T4 to T3 in addition to treating the relative adrenal insufficiency.
- PJP, formerly PCP pneumonia, is typically seen in those who are immunocompromised. The x-ray will have bilateral interstitial infiltrates in a bat wing configuration. If the PaO2 is less than 70 or the A-a gradient is greater than 35, treat with steroids in addition to trimethoprim-sulfamethoxazole.
So, that wraps up Episode 25. Do not forget to listen for the trauma phone ring tone in the coming weeks for a chance to win a Rosh Review Subscription. Remember to tweet (@Roshcast) or email (Roshcast@roshreview.com) the exact time you hear the ring to win the prize.
Until next time,
Jeff and Nachi

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Comments (0)