
Podcast Ep 33: Heart Block, Hypothermia, Bullous Myringitis, & More



People who are crazy enough to think they can change the world, are the ones who do.
-Rob Siltanen
Welcome back to Roshcast Episode 33! This episode marks an incredible milestone for Roshcast. Exactly 365 days ago, Roshcast was born (Apgars 7 and 9). It is wild to look back and think about how much we have covered – hundreds of questions, thousands of pearls, dozens of test-taking strategies, regular tweets, etc.
We couldn’t be more excited about where Roshcast has been or where it is going. In honor of hitting one year, we are doing another trauma ring tone competition. During episodes 34 to 38, listen for a trauma ring tone, and tweet the exact time to us or e-mail the time to us. A few weeks ago, we also launched a new partnership with the EM Clerkship podcast as a core EM corollary for selected topics. This week, we are doing another crossover episode, in which we return to cardiac arrhythmias — specifically, bradycardia. Let’s get the episode started with a rapid review of some essential vitamins, which were recently covered on the Rosh Blog.

- The fat-soluble vitamins are A, D, E, and K.
- Vitamin D deficiency can lead to rickets in children and osteomalacia in adults. Vitamin D deficiency is classical seen in the elderly, those with insufficient sun exposure, malnutrition, malabsorption, breastfeeding infants, and those who take anticonvulsants.
- Vitamin E deficiency can present with areflexia, peripheral neuropathy, gait abnormalities, ophthalmoplegia, and decreased proprioception.
- Vitamin A deficiency is associated with night blindness, xerosis (dryness of the skin, mucous membranes, and conjunctiva), as well as Bitot’s spots (white patches on the conjunctiva).
Now onto this week’s podcast
Question 1
A 66-year-old woman presents with generalized weakness and dyspnea on exertion for 2 weeks. Vital signs are BP 80/45, HR 40, RR 16, and pulse oximetry 97% on room air. Her ECG is shown above. There are no other ST-segment abnormalities. Which of the following is the most appropriate next step in management?
A. Administer aspirin, heparin and admit for acute coronary syndrome
B. Cardiac catheterization laboratory activation
C. Observation and arrange for follow up with cardiology
D. Place a transcutaneous pacemaker
Question 2
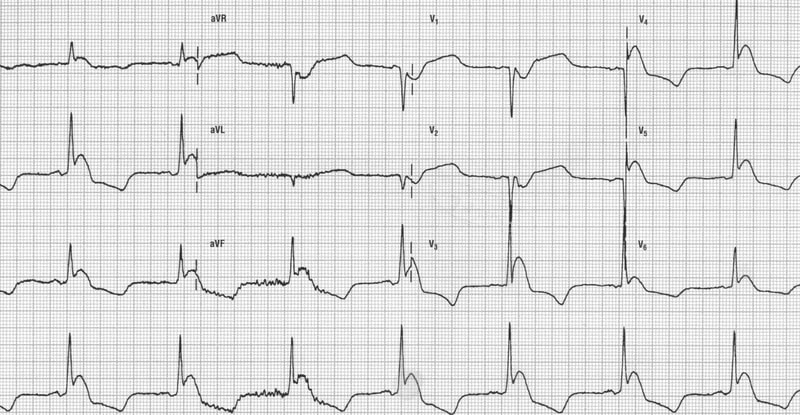
A patient has the above ECG shown above. Which of the following findings is likely to be present on exam?
A. A harsh crescendo-decrescendo systolic murmur
B. A swollen and tender right lower leg
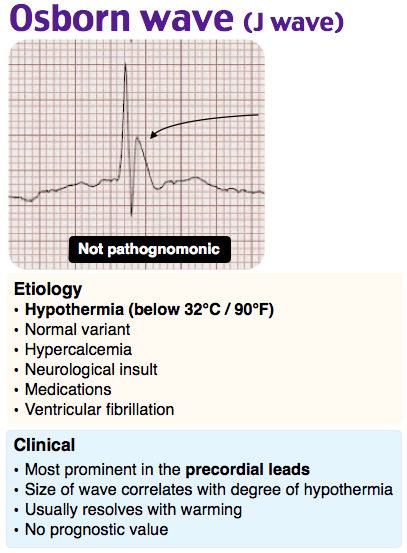
C. Decreased core body temperature
D. Elevated jugular venous distension
Question 3
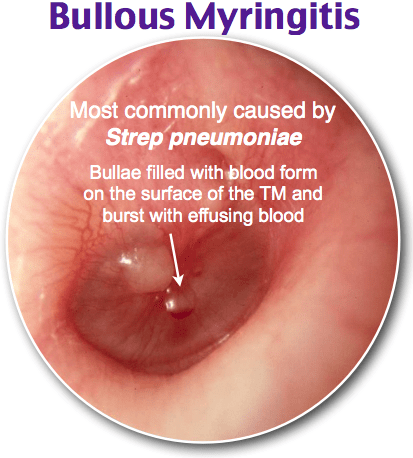
Which of the following organisms is associated with pneumonia and bullous myringitis?
A. Bordetella pertussis
B. Haemophilus influenzae
C. Streptococcus bovis
D. Streptococcus pneumoniae
Question 4

A 52-year-old man presents from his primary care physician’s office for evaluation of an abnormal electrocardiogram. His ECG is seen above. He has no symptoms. What is the appropriate intervention?
A. Measurement of cardiac enzymes
B. No intervention
C. Telemetry observation
D. Transcutaneous pacer pad placement
Question 5
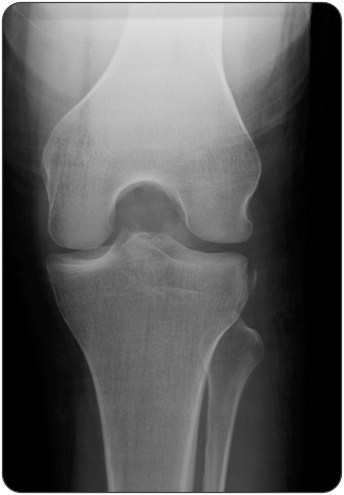
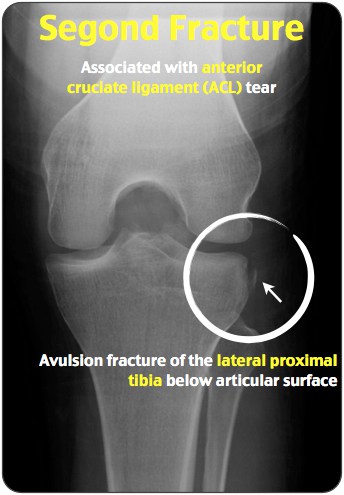
A Segond fracture, seen in the X-ray above, is pathognomonic for what ligamentous injury?
A. Anterior cruciate ligament (ACL)
B. Lateral collateral ligament (LCL)
C. Medial collateral ligament (MCL)
D. Posterior cruciate Ligament (PCL)
Question 6
An infant with episodes of cyanosis and respiratory difficulty is diagnosed with Tetralogy of Fallot. Which of the following defects would you expect to see on echocardiographic examination?
A. Aorta-pulmonary artery transposition
B. Atrial septal defect
C. Left ventricular hypertrophy
D. Overriding aorta
Question 7
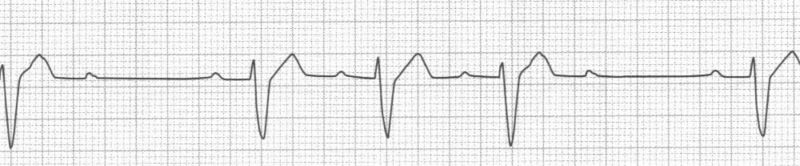
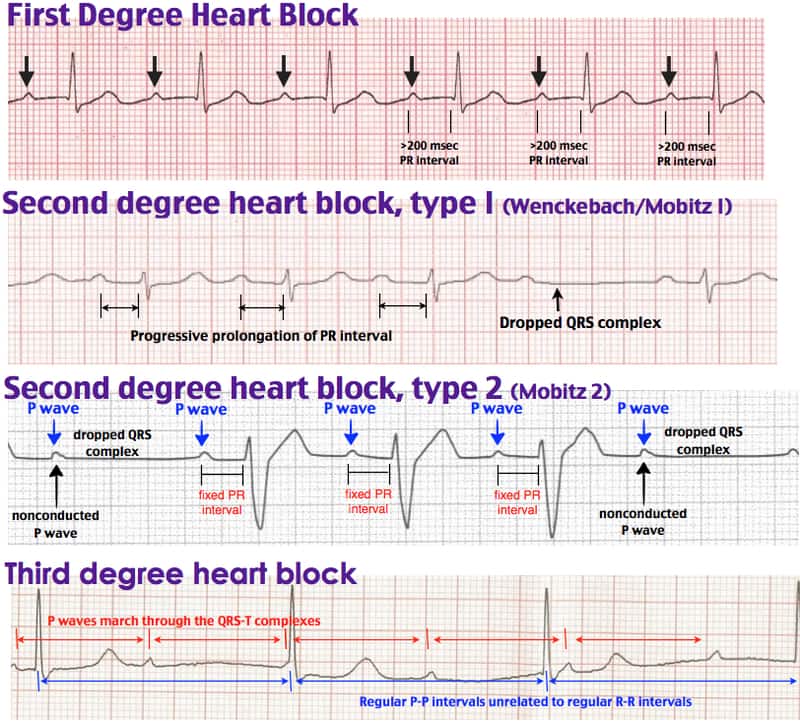
A 50-year-old woman presents to the ED with minor chest pain. She lifted some heavy groceries from the car yesterday. She has a history of hypertension that is controlled with metoprolol. In the ED, her vital signs are BP 120/80, HR 68, RR 14, and oxygen saturation 99% on room air. Her rhythm strip is seen above. Which of the following is the represented rhythm?
A. First-degree heart block
B. Third-degree heart block
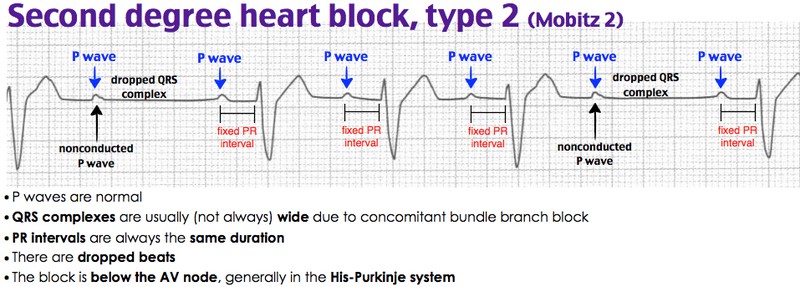
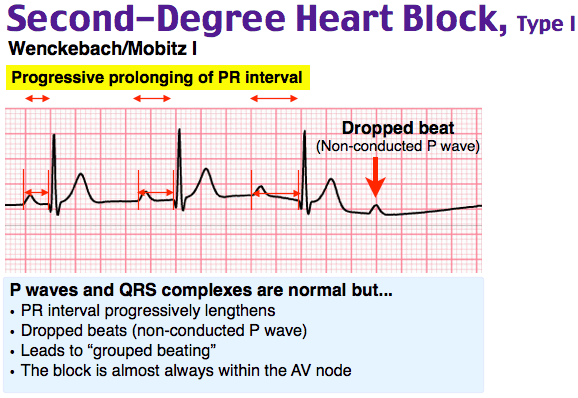
C. Type I second-degree heart block
D. Type II second-degree heart block
- Second-degree type 1 block may be related to increased vagal tone or medications that block the AV node.
- Second-degree type 2 block and complete heart block require a pacemaker. If symptomatic or hemodynamically unstable, patients with such high degree AV block require immediate transcutaneous or transvenous pacing until a permanent pacer can be implanted.
- Medications that block the AV node include adenosine, beta-blockers, calcium channel blockers, and digoxin.
- Osborn waves, also known as late delta waves or J waves, are positive deflections of the J point that are characteristic of hypothermia and are usually only seen at temperatures below 32° Celsius.
- Concurrent bullous myringitis and pneumonia is associated with Streptococcus pneumoniae. Treating the pneumonia will also treat the otalgia.
- A Segond fracture is pathognomonic for ACL injury.
- To test for ACL injury, perform either the Lachman or the anterior drawer test. The Lachman test is more sensitive.
- Remember the PROVe mnemonic for the cardiac defects seen in Tetralogy of Fallot (ToF): Pulmonary stenosis, RV hypertrophy, Overriding aorta, and VSD.
That wraps up Episode 33, marking one full year of Roshcast. We will be at ACEP at the end of the month and hope to see many of you there. Definitely swing by the Rosh Review booth (1442) to say hi and give us some feedback or any suggestions you might have to improve the podcast! Don’t forget to follow us on Twitter @Roshcast and @Roshreview. We can also be reached by email at roshcast@roshreview.com. Remember that you can help us pick questions by identifying ones you would like us to review. To do so, write “Roshcast” in the submit feedback box as you go through the question bank. And finally, if you have a minute, make sure to rate us and leave comments on iTunes to help spread the word about Roshcast.
Until next time,
Jeff and Nachi

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Comments (0)