
Podcast Ep 40: Croup, Trigeminal Neuralgia, PJP Pneumonia, & More




Dreams and dedication are a powerful combination.
-William Longgood
Welcome back to Roshcast for Episode 40! After a quick detour last week to talk with Dr. Rosh, we are back at it with our regular routine. But before we get going, if you have any thoughts or feedback on last week’s episode, or even if you have any unanswered questions, make sure you send them our way to RoshCast@RoshReview.com, so that we can get them answered either individually by email or on another special episode.
This week, we are going to cover a few pediatric respiratory questions to parallel the EM Clerkship podcast’s most recent episode in addition to some bread and butter emergency medicine. Before we begin, let’s get warmed up with a rapid review covering environmental emergencies, since these are things we see less frequently in our day to do practice but ALWAYS appear on the in-training exam.

- Pit viper bites cause local swelling and oozing from the wound. Severe envenomations can lead to a DIC like coagulopathy and hemorrhagic bullae.
- Brown recluse spider bites cause a papule that later blisters and may necrose. Systemic symptoms include renal failure, pulmonary edema, and shock.
- Black widow spider bites cause a local papule with a halo. Severe systemic symptoms include a peritonitic abdomen, muscle fasciculations, and diaphoresis. Remember that you can identify a black widow spider by the red hourglass on their abdomen.
- Frostbite should be treated with immersion in a warm water bath set at 37-39 degrees Celsius.
Now onto this week’s podcast
Question 1
Let’s get right into with a pediatric respiratory question: A 3-year-old girl presents to the ED with 1 hour of a barking cough and inspiratory stridor at rest. On exam, she has mild retractions but is not hypoxic. Which of the following interventions has been shown to reduce hospital length of stay in moderate to severe croup?
A. Dexamethasone
B. Heliox
C. Humidified air
D. Racemic epinephrine
Question 2
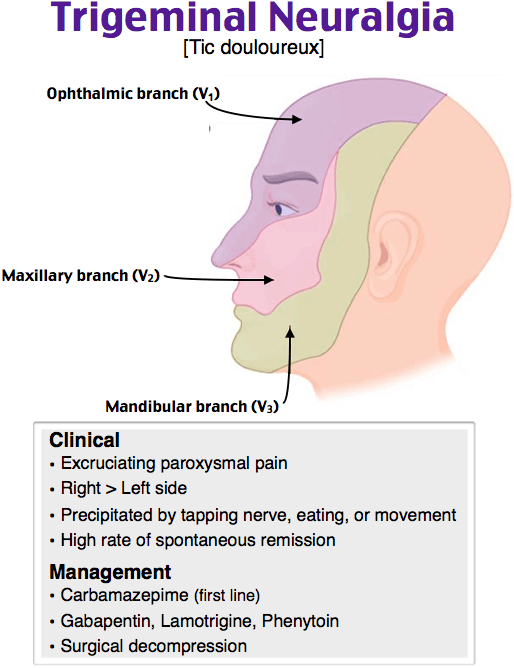
A 33-year-old woman presents with intermittent, intense shooting pain to the left side of the face. She states that the pain begins near her ear and radiates to her chin. The pain is often brought on by chewing and brushing her teeth. Which of the following managements is most likely indicated?
A. Carbamazepine
B. Dental X-rays
C. Mandible CT scan
D. Prednisone
Question 3
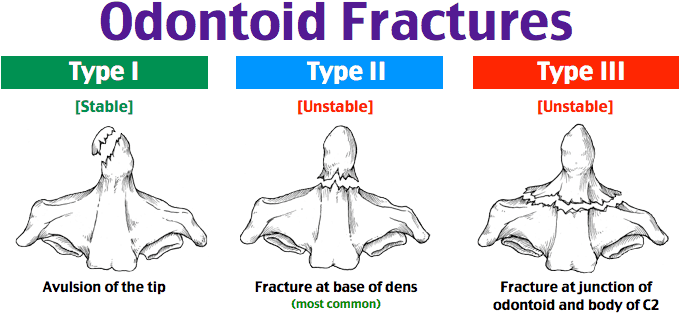
Which of the following cervical spine fractures is considered stable?
A. Bilateral facet dislocation
B. Flexion teardrop fracture
C. Jefferson fracture
D. Type I odontoid fracture
Question 4
You are working in a busy pediatric ED in December. During your shift, you evaluate and treat four children with moderate croup by administering oral dexamethasone and aerosolized epinephrine. You re-evaluate each child two hours after the initial racemic epinephrine treatment. Which of the following children can most safely be discharged home?
A. A 1-year-old boy with persistent stridor at rest
B. A 2-year-old uninsured boy with clinical improvement, but no primary care physician
C. A 3-month-old girl with a history of tracheomalacia who has clinical improvement
D. A 4-year-old girl with retractions that have since resolved
Question 5
A 10-year-old boy presents with increased lethargy and vomiting. Mom states the patient has had three days of cough, rhinorrhea, sore throat, and fever. The nanny has been giving the patient an appropriate dose of over-the-counter cold medicine. The physical exam is remarkable for lethargy, mild icterus, and hepatomegaly. Laboratory results are remarkable for markedly elevated AST and ALT. Which medication is most likely responsible for this patient’s presentation?
A. Acetaminophen
B. Aspirin
C. Guaifenesin
D. Ibuprofen
Question 6
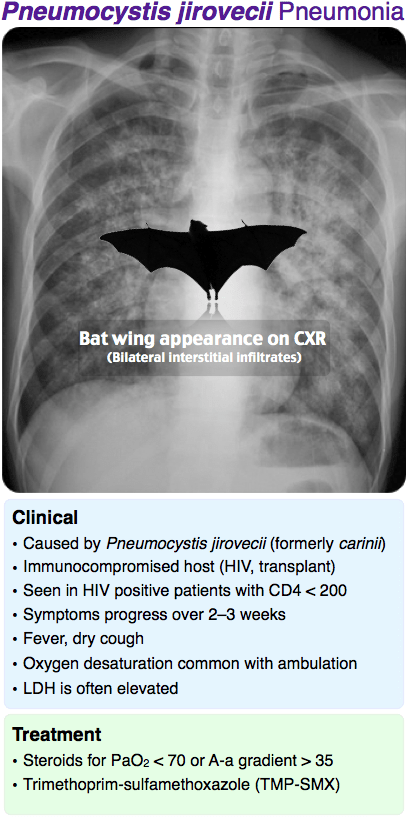
A 52-year-old man with a history of renal failure status post-transplant presents with shortness of breath. He has had a non-productive cough with fevers for the last 3 days. His only medication is mycophenolate mofetil. With ambulation, he desaturates to 85% on room air and his resting saturation is 90%. Physical examination is notable for diffuse bilateral crackles. His chest X-ray is shown above. Which of the following is the most appropriate drug to administer next?
A. Anaerobic antibiotic coverage
B. Beta-agonist
C. Loop diuretic
D. Oral corticosteroid
Question 7
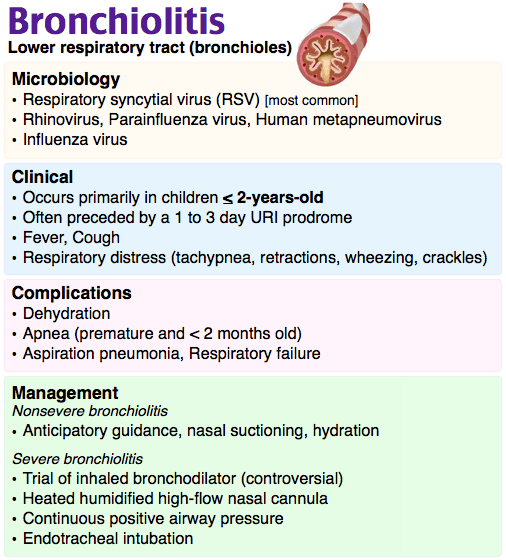
A 6-month-old girl born at 35 weeks gestation and previously well presents to the ED with wheezing and increased work of breathing. Mom reports that her daughter has had a low-grade fever, rhinorrhea, and cough for the past 3 days. In the ED, the patient’s vital signs are T 38.3ºC, HR 150/min, RR 72/min, and a pulse oximetry of 90% on room air. On exam, she is wheezing, using accessory muscles, and having subcostal retractions. An albuterol nebulizer treatment was given but no improvement was seen. Which of the following is the most appropriate next step in management?
A. Administer 1 mg/kg of oral dexamethasone
B. Administer another albuterol nebulizer treatment because the patient continues to be wheezing
C. Administer high-dose inhaled corticosteroids
D. Admit to the hospital and provide supportive care
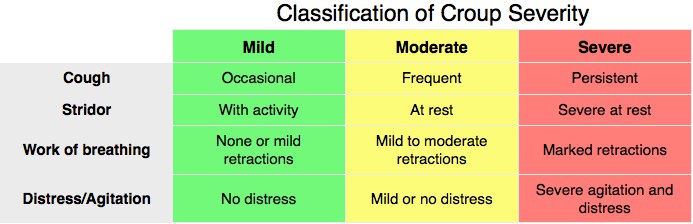
- Dexamethasone is the first-line treatment for croup. It reduces hospital length of stay in moderate to severe case of croup.
- The Westley Croup Severity Score incorporates level of consciousness, cyanosis, stridor, air entry, and retractions to help guide management, which ranges from supportive care, to nebulized epinephrine, to ICU admission and intubation.
- In children with croup, chest X-ray may show the classic steeple sign.
- Trigeminal neuralgia presents with paroxysms of lancinating pain, typically in the V2 and V3 dermatomes. Treatment is with carbamazepine.
- Bilateral facet dislocations, flexion teardrop fractures, Jefferson fractures, and type 2 and type 3 odontoid fractures are all unstable cervical spine fractures.
- A flexion teardrop fracture is a fracture of the anterior inferior portion of the vertebral body, which disrupts the anterior and posterior ligamentous structures.
- A Jefferson fracture is a burst fracture.
- A type 1 odontoid fracture is an avulsion of the tip of the odontoid. A type 2 odontoid fracture, which is the most common, is a fracture at the base of the dens. A type 3 odontoid fracture is a fracture at the junction of the odontoid and the body of C2.
- Reye syndrome presents with a rapidly progressive, non-inflammatory encephalopathy associated with altered mental status, cerebral edema, and hepatic dysfunction. Patients typically present with respiratory or a GI prodrome followed by an encephalopathic picture.
- Reye syndrome is caused by salicylate usage in the setting of a viral illness. Influenza and chickenpox are commonly implicated viruses.
- PJP pneumonia presents with bilateral perihilar infiltrates in a classic batwing appearance. Immunocompromised patients are at risk.
- PJP pneumonia is ideally treated with trimethoprim-sulfamethoxazole. In sulfa allergic patients, consider primaquine-clindamycin or atovaquone for mild to moderate disease or pentamidine for severe disease.
- Bronchiolitis should be treated with supportive care. In first-time wheezers, evidence suggests that there is no role for oral steroids or beta-agonists.
That wraps up RoshCast Episode 40! Be sure to also check out the blog for questions from this episode and prior episodes, related images and tables, as well as bonus teaching points. There are also tons of other great free resources there to help prepare you for the boards and the wards. Don’t forget to follow us on Twitter @RoshCast and @RoshReview. You can always email us at RoshCast@RoshReview.com with any feedback, corrections or suggestions. You can also help us pick questions by identifying ones you would like us to review. Write “RoshCast” in the submit feedback box as you go through the question bank. Lastly, if you have a minute, make sure to rate us and leave comments on iTunes to help spread the word about RoshCast. We’ll be back soon with more high quality review.
Until next time,
Jeff and Nachi
Get Free Access and Join Thousands of Happy Learners

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
You must be logged in to post a comment.
Comments (0)