
Podcast Ep 36: Pediatrics, Chlamydial Pneumonia, & More




Do not go where the pay may lead, go instead where there is no path and leave a trail.
-Ralph Waldo Emerson
Welcome back to Roshcast Episode 36! This week we continue our collaboration with the EM Clerkship podcast, focusing on pediatrics. Don’t forget that we launched another trauma ring tone contest week, so listen up through Episode 38 to win a subscription to Rosh Review. For this week’s rapid review, we will be covering a few pearls from Yehuda’s most recent posts on the Rosh Review Blog. Let’s get started!

- Cysticercosis is caused by Taenia solium, a common tapeworm. It’s transmitted via pork. Patients may present with seizures and CNS cysts.
- Patients with acute angle-closure glaucoma classically present with severe eye pain, blurry vision, photophobia, and a dilated pupil. The intraocular pressure in this case would be elevated.
- Iritis presents with peri-limbic injection, a constricted pupil, pain, photophobia, and blurry vision. You would expect the intraocular pressure to be normal or even low.
Now onto this week’s podcast
Question 1
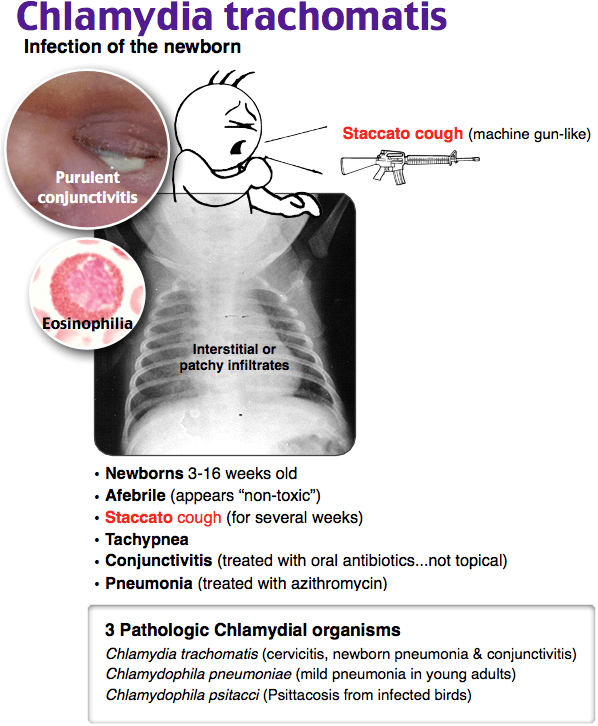
A 4-week-old boy presents with a 2-week history of increasing dyspnea, cough, and poor feeding. On examination you note conjunctivitis, and a chest examination reveals tachypnea and rales. A chest X-ray shows hyperinflation and diffuse interstitial infiltrates. Which of the following is the most likely etiologic agent?
A. Chlamydia trachomatis
B. Parainfluenza virus
C. Respiratory syncytial virus
D. Staphylococcus species
Question 2
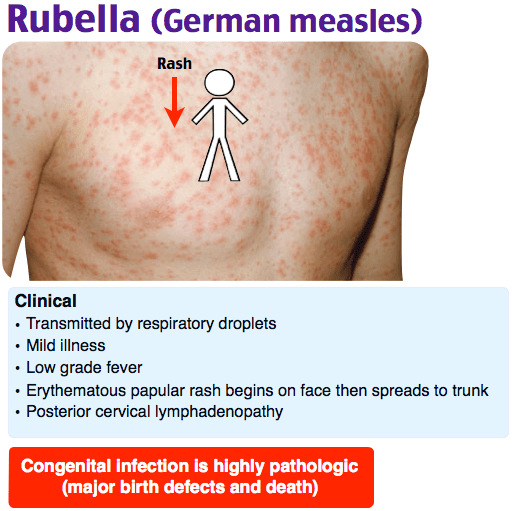
A 6-year-old immigrant boy from Bangladesh presents with fever and rash. The fever started three days ago followed by a rash which started on the head and spread to the rest of the body. Examination reveals a well-appearing child with a maculopapular rash and posterior cervical lymphadenopathy. Which of the following is the most likely causative organism for this disease?
A. Measles virus
B. Mumps virus
C. Parvovirus B19
D. Rubella virus
Question 3
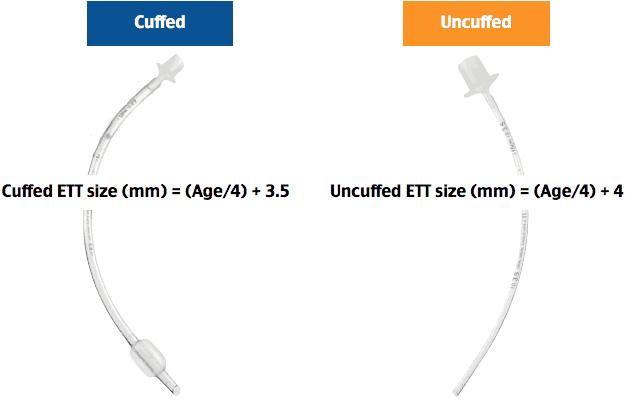
A 4-year-old boy presents with respiratory failure. Which of the following represents the correct endotracheal tube for this patient?
A. 4.0 cuffed endotracheal tube
B. 5.0 uncuffed endotracheal tube
C. 5.5 cuffed endotracheal tube
D. 6.0 cuffed endotracheal tube
Question 4
Which of the following is the most common manifestation of abusive head trauma in infants?
A. Epidural hematoma
B. Retinal hemorrhage
C. Subarachnoid hemorrhage
D. Subdural hematoma
Question 5
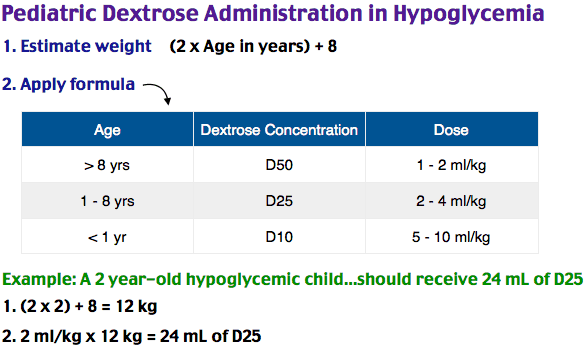
Which of the following should be administered to a symptomatic 3-day-old infant with glucose of 25 mg/dL?
A. 1 mL/kg of 50% dextrose (D50)
B. 2 mL/kg of 25% dextrose (D25)
C. 5 mL/kg of 10% dextrose (D10)
D. Glucagon subcutaneously
Question 6
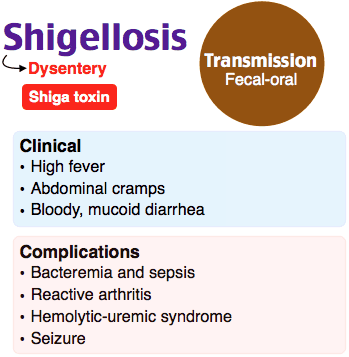
A healthy 6-year-old boy presents to the ED with bloody diarrhea. He was in his usual state of health until one week ago when loose, watery stools (up to 10 per day) were noted. He was seen by his pediatrician four days ago but has since developed increasing amounts of blood and pus in his stools along with a low-grade fever. Mom states there is no recent travel, antibiotic use, or known sick contacts. His vitals are heart rate 118 beats per minute, oxygen saturation 100% on room air, and rectal temperature of 38.3°C. Your physical exam reveals a mildly tender abdomen without localization, rebound, guarding, or peritoneal signs. You note grossly bloody stool on rectal exam. A brief discussion with his pediatrician confirms your suspicion of an invasive bacterial diarrhea; a stool culture was positive for Shigella. Which of the following statements is true regarding this condition?
A. Antibiotics should be avoided because this is a severe case and the patient is at highest risk of developing hemolytic uremic syndrome
B. Antidiarrheal agents (such as diphenoxylate and atropine) are indicated, given the frequency of loose stools
C. Extraintestinal manifestations such as hallucinations, confusion, and seizures may occur
D. Oral rehydration should be avoided; IV fluids should be initiated
- Chlaymdial pneumonia is often found in infants 3–16 weeks old. They usually present, non-toxic appearing and afebrile, but with tachypnea and a staccato cough, with or without rales. 50% also have conjunctivitis. Treat with azithromycin.
- Infants with parainfluenza virus typically present with coryza, a low-grade fever followed by a classic barking cough of croup.
- Infants with RSV present with lower respiratory tract infections like bronchiolitis.
- Measles presents with a fever followed by a rash and Koplik spots.
- Mumps is associated with an infectious parotitis.
- Infants with parvovirus B19 often present with erythema infectiosum with the classic slapped cheek appearance.
- Rubella, also called German measles, often presents with a mild febrile illness with a diffuse maculopapular rash, generalized malaise, along with lymphadenopathy.
- When choosing an endotracheal tube for children use the following formulas. For uncuffed tubes, take the age, divide it by 4, and add 4. For cuffed tubes, take the age, divide it by 4, and add 3.5.
- Retinal hemorrhages are the most common manifestation of abusive head trauma in infants.
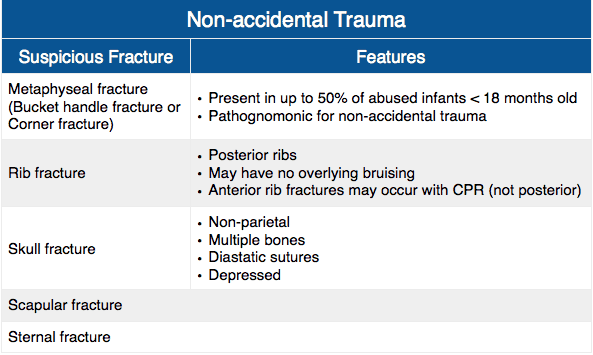
- Posterior rib fractures without overlying bruises, metaphyseal fractures, sternal fractures, scapular fractures, and skull fractures should raise your suspicion for non-accidental trauma.
- For hypoglycemic children less than one year of age, use D10 5–10 ml/kg. For hypoglycemic children who are 1 to 8 years old, use D25 2–4 ml/kg. For hypoglycemic children over the age of 8, use D50 1–2 ml/kg.
- Extraintestinal manifestations of Shigella include confusion, hallucinations, and seizures.
- For children concerning for shigellosis, treat supportively with PO fluids if tolerated. Antidiarrheal agents should be avoided. Depending on the situation, antibiotics may be needed.
That wraps up Episode 36. Don’t forget to follow us on Twitter @Roshcast and @RoshReview. We can also be reached by email at roshcast@roshreview.com and are open to any feedback, corrections, or suggestions. You can help us pick questions by identifying ones you would like us to review. To do so, write “Roshcast” in the submit feedback box as you go through the question bank. And finally, if you have a minute, make sure to rate us and leave comments on iTunes to help spread the word about Roshcast.
Until next time,
Jeff and Nachi
Get Free Access and Join Thousands of Happy Learners

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
You must be logged in to post a comment.
Comments (0)