
Everything You Need To Know for the Pediatric Hospital Medicine Certification Exam in 2024



Planning to take the Pediatric Hospital Medicine certification exam in 2024? Here’s what to know, including when to apply for the exam, what’s covered, and how to prepare.
When is the exam offered?
Every 2 years—the next examination will be offered on November 19–20, 2024.
When can I register?
Regular: February 5, 2024–April 1, 2024
Late: April 2, 2024–April 30, 2024
How many questions are on the Pediatric Hospital Medicine certification exam?
There are 200 multiple-choice questions, completed as a 4.5-hour proctored examination.
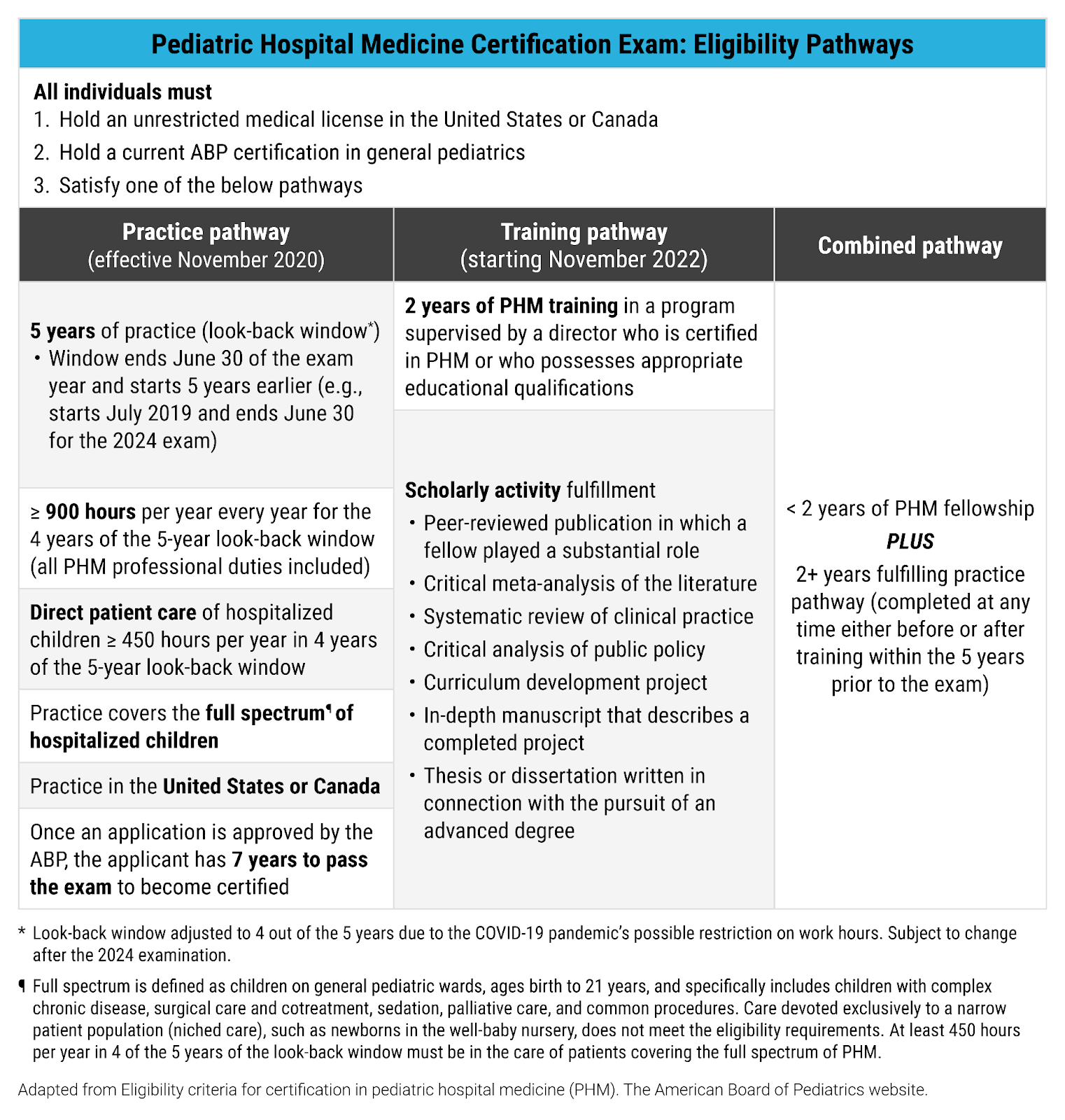
Who is eligible to take the exam?
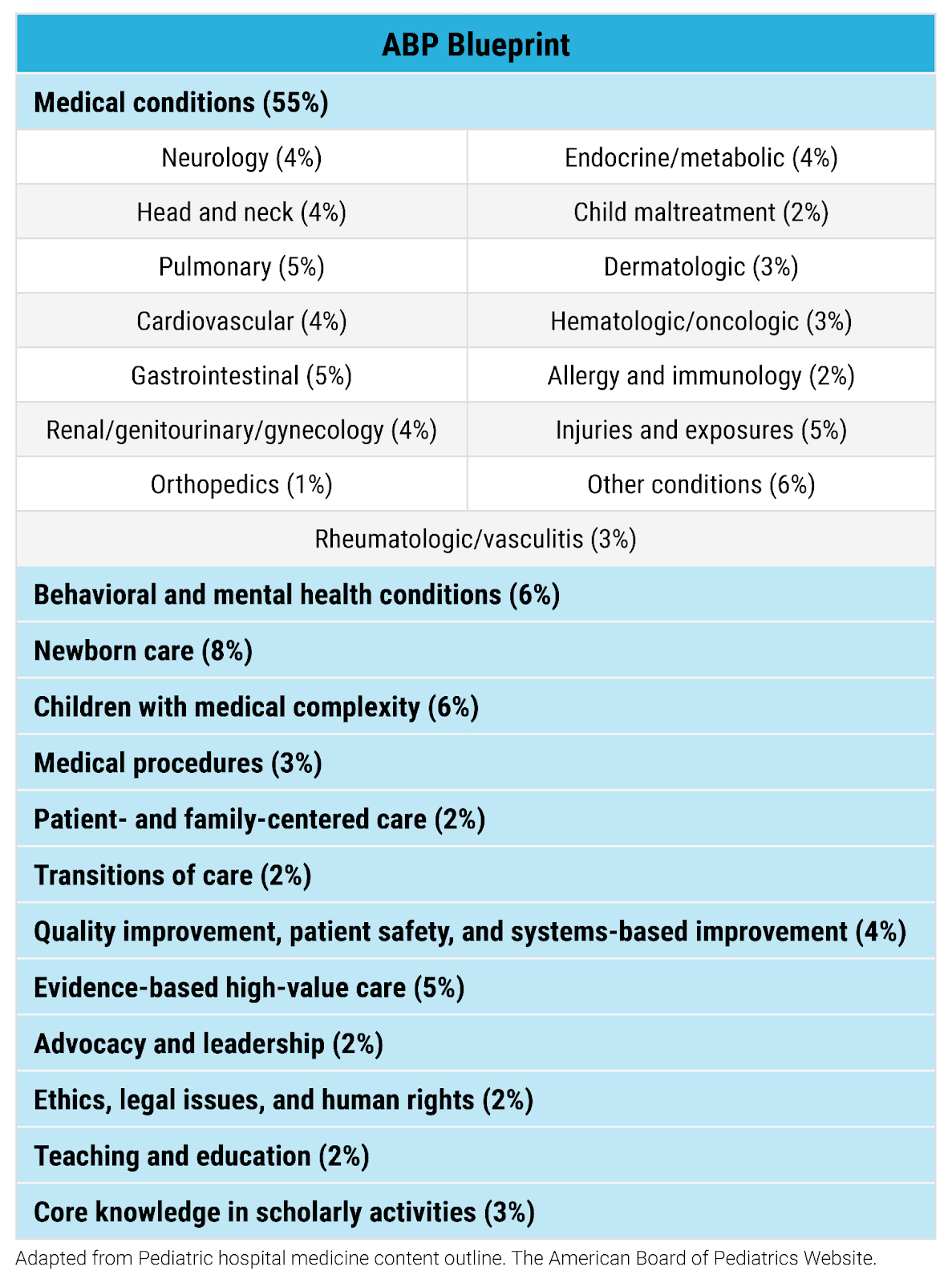
What content will be covered on the exam?
How do I study?
Preparing for medical board exams can be daunting, but with the right strategy and resources, you can be confident you’re doing it the right way. Begin by creating a study plan that divides the material into smaller sections. Concentrate on comprehending important concepts and principles instead of simply memorizing information.
While there are a few high-quality textbooks for pediatric hospital medicine, reading through them to study for the exam is not always practical. Practice questions are an essential part of your study plan for the boards. They help reinforce your understanding of the material, identify areas for improvement, and get you comfortable with the format of the exam.
That’s why, in keeping with our tradition of staying ahead of the curve, Rosh Review developed a comprehensive Pediatric Hospital Medicine Certification Qbank.
Just in time to supplement and consolidate knowledge acquired from the content in the Pediatric Hospital Medicine Certification Qbank, a brand-new, 100-question Pediatric Hospital Medicine Certification Mock Exam will be available this fall 2024! With these two options, you will be well-prepared for the examination in November.
Stay positive, stay focused, and believe in yourself. With the help of Rosh Review, success is within reach!
How many questions are in the Qbank?
The Rosh Review Pediatric Hospital Medicine Certification Qbank currently provides 550+ ABP board-style questions with comprehensive explanations for both the correct and incorrect answer choices, beautiful images that highlight key learning points, and Rapid Reviews to consolidate your knowledge.
The question bank was developed to align with the ABP content outline and covers core PHM medical content as well as topics such as evidence-based medicine, teaching, ethics, advocacy and leadership, quality improvement, and patient safety.
Who developed the content?
Our author team is composed of clinically experienced, board-certified general pediatricians and board-certified pediatric hospitalists who are up-to-date with current clinical practice guidelines.
All the content is reviewed by a board-certified pediatric hospitalist and undergoes a rigorous editing process. If you’d like to learn more about how a Qbank is made, check out this post about How a Rosh Review Qbank is Made: Our Question Writing and Editing Process.
What does a sample question look like?
Questions are vignette-based ABP format. Here is an example question:
A 4-year-old boy is admitted for hydration in the setting of inadequate oral intake, low-grade fever, and malaise. He has a history of cerebral palsy, global developmental delay, and epilepsy secondary to perinatal ischemia. His epilepsy has been difficult to control, and lamotrigine was added to his antiepileptic regimen 3 weeks ago. Sick contacts include a brother who required a recent incision and drainage of a cutaneous abscess. On the day after admission, he developed an erythematous macular rash on his face. The macules then coalesced and spread down his body. The lesions on his face developed into bullae, which ruptured and left behind large, tender ulcerations. In addition, he has developed bilateral conjunctivitis with scant exudate, as well as oral ulcers. Which of the following is indicated in further evaluation?
A. Complete blood count with differential to evaluate for drug reaction with eosinophilia and systemic signs
B. Comprehensive metabolic panel to evaluate for systemic effects of Stevens-Johnson syndrome
C. Laboratory evaluation to support a diagnosis of atypical Kawasaki disease
D. Wound cultures of intact bullae for Staphylococcus aureus sensitivities
What do the detailed explanations look like?
Explanations provide a comprehensive review of the topic so you’ll take away all of the high-yield, critical information to succeed on the exam. You’ll note high-yield terms and other important phrases are bolded.
Additionally, knowing why the correct answer is correct is important, of course. But knowing why the incorrect answer choices are incorrect is just as valuable. Every incorrect answer choice in the Qbank is explained so you understand the nuances of the topic and also learn about related topics.
For example, the answer to the above questions is choice B. Here is the detailed explanation for both the correct answer and incorrect answers:
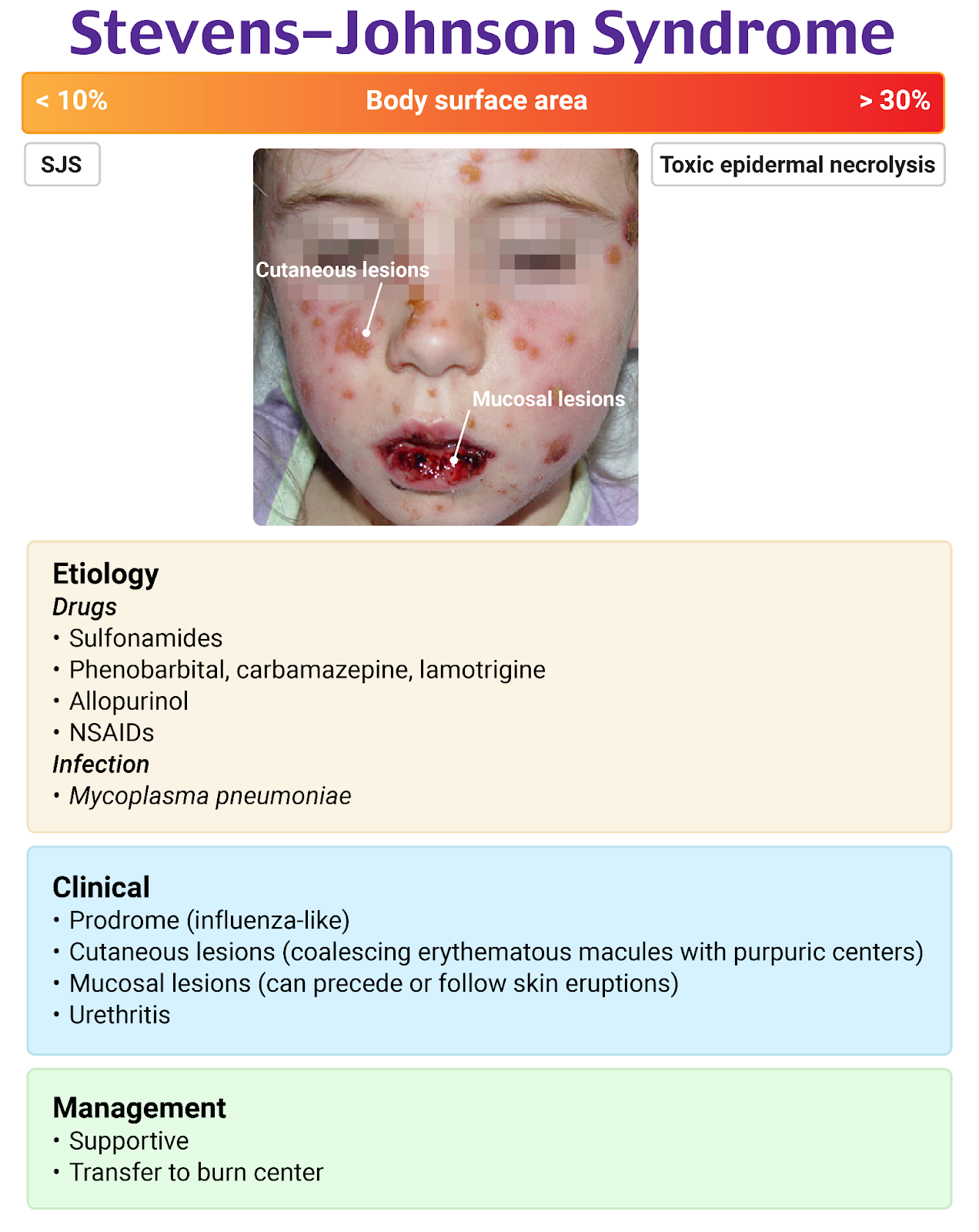
This child has a history of a hypoxic-ischemic event in the perinatal period and has resulting cerebral palsy, global developmental delay, and epilepsy with a recent addition of lamotrigine to his antiepileptic regimen. He initially presented with a nonspecific prodrome of low-grade fever and decreased oral intake, but he has developed an impressive exanthem and enanthem. The exanthem progressed from a facial rash to a more diffuse rash that is evolving from macules and erythroderma to bullae and large erosions. In addition, he has exudative conjunctivitis, and oral ulcers. His presentation is most consistent with Stevens-Johnson syndrome or toxic epidermal necrolysis; the distinction depends on the percentage of body surface area that is affected by the rash. Stevens-Johnson syndrome refers to blistering and ulcerations that affect less than 10% of body surface area, while toxic epidermal necrolysis affects greater than 30% of body surface area.
Medications are the most common trigger for Stevens-Johnson syndrome, and antiepileptic drugs such as lamotrigine, carbamazepine, and phenobarbital are well-recognized triggers. Sulfa drugs and infection with Mycoplasma pneumoniae are frequently associated with Stevens-Johnson syndrome. A skin biopsy may be used to confirm a suspected diagnosis and to exclude alternative etiologies of the exanthem.
The laboratory evaluation of Stevens-Johnson syndrome should include a comprehensive metabolic panel to evaluate both liver and renal function since both may be affected. Additional laboratory evaluation should include a complete blood count, inflammatory markers, and serologies and titers for M. pneumoniae. In addition, cultures of open wounds, oral lesions, and blood should be performed due to risk of bacterial superinfection. Patients with Stevens-Johnson syndrome are also at risk of mucosal involvement of the gastrointestinal tract, including the esophagus, small bowel, and colon. Due to the high risk of pneumonia and interstitial pneumonitis, chest radiography should be obtained in all children who also present with pulmonary symptoms.
Treatment of Stevens-Johnson syndrome is supportive and includes immediate discontinuation of the offending agent, provision of hydration, correction of electrolyte disturbances, nutritional support, wound care, ophthalmologic care, pain control, and treatment of superinfections.
Antiepileptic medications may also precipitate drug reaction with eosinophilia and systemic signs (DRESS), which can present soon after initiation of new medications such as carbamazepine, lamotrigine, phenobarbital, or phenytoin. In contrast to Stevens-Johnson syndrome, DRESS less commonly causes mucosal involvement. If present, mucosal lesions typically do not ulcerate. A complete blood count with differential to evaluate for drug reaction with eosinophilia and systemic signs (A) is unlikely to demonstrate eosinophilia. Stevens-Johnson syndrome is not associated with eosinophilia, but leukopenia and anemia are often present.
A laboratory evaluation for atypical Kawasaki disease (C) is not indicated. Though this child does have a fever, a diagnosis of Kawasaki disease requires at least 5 days of fever. In addition, the conjunctivitis of Kawasaki disease is nonexudative, and the oral findings do not typically include ulcerations. Though the rash of Kawasaki disease may have a variety of appearances, it does not typically include bullae or ulcerations.
Staphylococcal scalded skin syndrome is an important differential diagnosis for Stevens-Johnson syndrome, and the child does have recent exposure to a brother with a skin infection, which raises suspicion for exposure to Staphylococcus aureus. However, the progression and distribution of the child’s rash in the setting of recent antiepileptic initiation, as well as his oral ulcerations, are not characteristic of staphylococcal scalded skin syndrome. As such, evaluation for staphylococcal scalded skin syndrome is not indicated. Moreover, wound cultures of intact bullae for Staphylococcus aureus sensitivities (D) are not useful in the evaluation of staphylococcal scalded skin syndrome, as the bullae contents are sterile.
At the end of each question, you are provided with another question related to the main topic to help reinforce what you just read. This is called the One Step Further question.
Try this:
Which laboratory tests should be obtained to evaluate for incomplete Kawasaki disease?
And the answer is:
C-reactive protein, erythrocyte sedimentation rate, complete blood count, albumin, alanine aminotransferase, and urinalysis.
Have you had enough? There’s more! Before you move on to the next question, you can read through the Rapid Review, which summarizes the key elements of the topic. In this case, Stevens-Johnson syndrome.
Stevens-Johnson Syndrome
- PE: vesicles and bullae involving < 10% of the body surface area, including mucous membranes
- > 30% BSA – Toxic epidermal necrolysis (TEN)
- Cause: sulfonamides, NSAIDs, AEDs, M. pneumoniae
- Tx: wound care, intravenous fluids (using Parkland formula), optimize nutrition, pain control, burn center
Now you’re ready!
You should leave this question with a firm understanding of how to answer questions about Stevens-Johnson syndrome correctly on the Pediatric Hospital Medicine Certification exam.
Since there are other options to help you prepare for the Pediatric Hospital Medicine Certification exam, before you decide to spend money with Rosh Review, get your free trial to the Pediatric Hospital Medicine Certification Qbank and get a better idea if this Qbank is right for you.
Please let us know if you have any questions. Reach out by emailing info@blueprintprep.com for insights about preparing for the Pediatric Hospital Medicine Certification exam or about any of Rosh Review’s Qbanks.
Get Free Access and Join Thousands of Happy Learners

You must be logged in to post a comment.
Comments (0)