
How to Crush Your Family Medicine Shelf Exam, and Other Insider Tips

Related Articles


It’s finally time for your family medicine rotation and you could not be more excited. Although you’re not interested in primary care, you just completed your surgery rotation and are desperately in need of sleep. A month of outpatient nine-to-five clinic visits doing well-child visits and reassuring patients that they don’t need antibiotics to treat a viral cold sounds like a piece of cake.
On your first day of the family medicine rotation, you show up for clinic already loving this new gig. Your alarm didn’t go off until 8:15 AM (!) and you even had time to stop for coffee and breakfast on the way. You think that you must be living the dream until your attending assigns you to a schedule of patients and reminds you not to dilly dally since each visit is only 15 minutes (including the time to write the note). Oh, and she almost forgot, some slots are double booked. Maintain professionalism and be efficient, you are warned, otherwise you’ll all be working through lunch. “No big deal, I got this,” you say to yourself. After all, you are a confident and competent third-year medical student who has already completed the majority of your clinical rotations and have done stellar on your shelf exams. How hard could this be?
As you race between rooms, your ability to rapidly access your clinical knowledge will be put to the test:
- On a pediatric knee exam, does a Lachman test evaluates the anterior cruciate ligament or meniscus? Do you know how to perform a McMurray test?
- Next, a 30-year-old G2P1 woman presents for screening for gestational diabetes. You know that the diagnosis requires a 2-step approach with a 1-hour venous glucose measurement following a 50-gram oral glucose solution, followed by a 3-hour oral glucose tolerance test, but does the diagnosis require 2 abnormal values on the 3-hour test or just 1?
- Before having a chance to look up the answer, your next patient (who has been waiting for over an hour) is a 78-year-old man with a complex medical history who takes furosemide, metformin, warfarin, pantoprazole, levothyroxine, sertraline, and aripiprazole. His caregiver says that he has had an altered mental status over the past three days. Your differential is so long that you could spend the rest of the afternoon drawing labs and ordering tests to evaluate him.
On a day like this, not only will you be missing lunch, but your confidence level might drop by the minute.
Welcome to your Family Medicine rotation. Jack of all trades.
If, like many students, you’re asking “How will I crush my family medicine rotation and get a top score on my family medicine shelf exam without having to rewatch all of my medical lectures on two speed?” Don’t worry—we’ve got you covered.
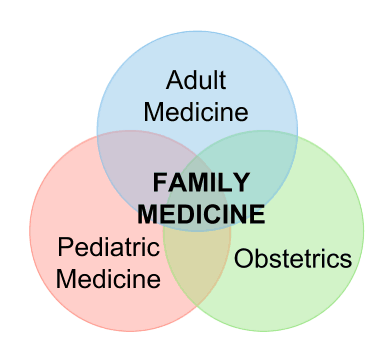
Before getting into the nitty-gritty details about whether to use azithromycin or doxycycline to treat chlamydia, you absolutely must take a step back and get a bird’s-eye view to understand the role of a family medicine physician within the health care system. While you are responsible for knowing about the diagnosis and management of complex disease processes, remember: the clinical rotation and family medicine shelf exam do not expect you to be an expert.
Family medicine requires you to be able to efficiently and effectively identify the difference between a patient who presents with a dull pain in the mid-abdomen that becomes sharp as it moves to the lower right abdomen with associated nausea and fever as a potential appendicitis requiring an emergent diagnostic workup, versus a patient with a stomachache who presents after eating too much at Thanksgiving dinner and will be better the next morning.
What kind of information should you know for the shelf exam?
The family medicine shelf is built to test your ability to differentiate patients who require urgent attention versus those who do not. Are you able to identify from the hints in the question stem, such as the instability of vitals or acuity of onset of symptoms, if this is a patient who can be scheduled at 4 PM next week, should be accessed in the clinic right now, or taken by an ambulance to the emergency room for an immediate evaluation? As a family medicine provider, you are the gatekeeper to the health care system, and question banks and shelf exams test your ability to know what you can manage on your own in a clinic setting versus who needs to be seen by an expert or specialist.
While the family medicine shelf exam will expect you to correctly diagnose primary hypertension according to national guidelines and select the first-line antihypertensive agents in a patient given their age, race, and comorbidities, you do not need to be able to manage an ICU patient who is in a hypertensive crisis following a craniotomy…we’ll leave that to the brain surgeons. This may seem like a simple concept, but if you stick to it you’ll have a much easier time focusing your attention on what the scenarios on the pediatric shelf exam are going to present you with.
While preparing for your clinical rotation and your family medicine shelf exam, recognize that a major role of a family medicine physician is not only to treat patients on an individual level, but to manage population-based care incorporating screening and vaccination guidelines. For example, the exam will likely test your knowledge on colorectal cancer screening. You must be able to risk stratify a patient and identify who, when, and how the screening should be performed. The same is true of screening for breast cancer, cervical cancer, diabetes, cholesterol, hepatitis C and lead poisoning.
This is also true for vaccinations. By the time you sit down to take your family medicine shelf exam, you are expected to know what the recommendations are for HPV, pneumococcus, varicella-zoster, meningitis, and hepatitis, among others. After all, you are the one who is responsible for carrying out the screening and vaccination guidelines for newborns and every age until the end of life. It is your job to detect who would benefit from lifestyle, dietary, or pharmacologic interventions in an attempt to prevent illnesses and disease complications that result in the need of a specialist.
Keep an eye out for zebras
The term “zebra” is medical slang for arriving at an exotic medical diagnosis when a more commonplace explanation is more likely. The term was coined by Dr. Theodore Woodward, who instructed his interns, “When you hear hoofbeats, think of horses, not zebras.” Keep this in mind on your family medicine rotation and shelf exam. The goal is to identify most patients as “horses” and to know that when you come across a suspected “zebra,” you can always refer to a specialist.
Get your free trial to the best Family Medicine Qbank to help you crush your shelf exam.
This is what one of your colleagues had to say about Rosh Review’s Family Medicine Qbank:
“Hands down the best Family Medicine Qbank from soup to nuts. Your explanations are incredibly high yield and taught me exactly what I needed to know for the Shelf Exam. The customer service is amazing, too. I had a few questions about the content and received personal responses within two hours of my email. Your team is truly amazing.”
– Stephanie Daniels, MD
You may also find the article How to Increase Your Family Medicine Certification Exam Score by 100 points useful. It’s never to early to prepare for your boards!
Get Free Access and Join Thousands of Happy Learners

You must be logged in to post a comment.
Comments (0)