
700 New Questions Just Added to the Internal Medicine Qbank



We just added 700 new questions, comprehensive explanations, teaching images, One Step Further™ questions, and Rapid Reviews to the Internal Medicine Certification Exam Qbank, bringing the total to more than 3,100!
Here’s a peek at one of the new questions:
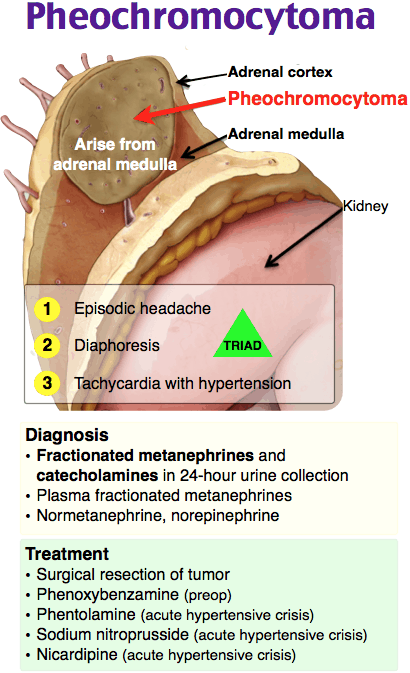
A 50-year-old man presents to his primary care physician complaining of intermittent episodes of tachycardia, hypertension, sweats, and headache. An extensive workup reveals increased 24-hour urinary fractionated metanephrines. A 3 cm adrenal mass consistent with a pheochromocytoma without malignant features is visualized on CT scan. After surgical consultation, a laparoscopic adrenalectomy is planned in 10 days. He has no significant past medical history and does not take any medications. Which of the following is the most appropriate next step in management?
A. Initiate both metoprolol and phenoxybenzamine now
B. Initiate metoprolol now and phenoxybenzamine 3 days prior to surgery
C. Initiate phenoxybenzamine now and metoprolol 3 days prior to surgery
D. No medication therapy is necessary
Answer: C
The most appropriate next step is to initiate phenoxybenzamine now and metoprolol 3 days prior to surgery. A pheochromocytoma is a neuroendocrine tumor originating from the chromaffin cells of the adrenal medulla. Pheochromocytomas are rare tumors that can arise sporadically from a de novo mutation or can be associated with a familial syndrome, such as von Hippel-Lindau syndrome or multiple endocrine neoplasia type 2. Pheochromocytomas produce at least one catecholamine (epinephrine, norepinephrine, or dopamine). Classic presentation involves intermittent tachycardia, sweats, headaches, and episodic or persistent hypertension. Radiologic evaluation with CT or MRI should be performed in patients whose biochemical testing with either plasma metanephrines or 24-hour urinary metanephrines is indicative of a pheochromocytoma. Patients with pheochromocytomas should undergo surgical resection, with laparoscopic adrenalectomy preferred for patients with single, small intra-adrenal tumors without malignant features. Preoperative medical therapy is necessary to manage tachycardia and hypertension (preventing a hypertensive crisis in surgery) and to expand volume prior to surgery. An alpha-adrenergic blocker, such as phenoxybenzamine, is recommended for 7–10 days prior to surgery. A beta-blocker, such as metoprolol, is started 2–3 days prior to surgery, but only after alpha-adrenergic blockade has been established to prevent unopposed alpha-adrenergic receptor stimulation.
Initiate both metoprolol and phenoxybenzamine now (A), initiate metoprolol now and phenoxybenzamine 3 days prior to surgery (B), and no medication therapy is necessary (D) are incorrect. This patient requires medical therapy prior to surgery. Preoperative beta-blockers should not be administered until alpha-adrenergic blockade has been achieved. Worsening hypertension can develop if vasodilatory peripheral beta-adrenergic receptors are blocked while there is unopposed alpha-adrenergic receptor stimulation.
Work hard, stay focused, and know Rosh Review is always by your side.
Best,
The Rosh Review Team
P.S. For tips about studying for the ABIM Certification Exam, check out How to Boost Your ABIM Internal Medicine Certification Exam Score by 100 Points.
Get Free Access and Join Thousands of Happy Learners

You must be logged in to post a comment.
Comments (0)