
Announcing the First-Of-Its-Kind Journal Club Qbank

Related Articles



We all know that journal club is a core component of residency education. New ideas for conducting journal club have certainly added to greater participation by residents (we think), made journal club more enjoyable (we hope), and led to greater retention and implementation of new knowledge (we pray).
Novel ideas for journal club are evident in sites like Wiki Journal Club, which provides free access to summarized clinical trials for readers around the world. But how can we elevate journal club even higher?
This may be what you’ve been looking for…
For the 2019–20 academic year, we’re providing free access to the first-of-its-kind Journal Club Qbank for programs that use Rosh Review.
We’ve taken 6 foundational EM journal club articles (more are being developed) and created vignette-style questions with comprehensive explanations and teaching diagrams.
Here are just a few of the benefits of the journal club module:
- Provide pretest and posttests journal club article assessments
- Allow residents who cannot attend journal club (e.g., those working overnights) the opportunity to engage in the article, and review its main points and take-aways despite being absent from the formal discussion
- Document participation and record time for asynchronous credit
Which articles did we start with?
- Article 1: The Atrial Fibrillation Follow-Up Investigation of Rhythm Management (AFFIRM) Investigators. A comparison of rate control and rhythm control in patients with atrial fibrillation. N Engl J Med. 2002;347(23):1825–1833. Download
- Article 2: ProCESS Investigators, Yealy DM, Kellum JA, Huang DT, et al. A randomized trial of protocol-based care for early septic shock. N Engl J Med. 2014;370(18):1683–1693. Download
- Article 3: Parienti JJ, Mongardon N, Megarbane B, et al. Intravascular Complications of Central Venous Catheterization by Insertion Site. N Engl J Med 2015;373:1220–1229. Download
- Article 4: Hoffman JR, Wolfson AB, Todd K, Mower WR. Selective Cervical Spine Radiography in Blunt Trauma: Methodology of the National Emergency X-Radiography Utilization Study (NEXUS). Ann Emerg Med. 1998;32(4):461–469. Download
- Article 5: Smith-Bindman R, Aubin C, Bailitz J, et al. Ultrasonography versus Computed Tomography for Suspected Nephrolithiasis. N Engl J Med. 2014; 371:1100–1110. Download
- Article 6: CRASH-2 trial collaborators, Shakur H, Roberts I, et al., Effects of tranexamic acid on death, vascular occlusive events, and blood transfusion in trauma patients with significant haemorrhage (CRASH-2): a randomised, placebo-controlled trial. Lancet. 2010;376(9734):23–32. Download
Here is what a question and explanation looks like from Article 1:
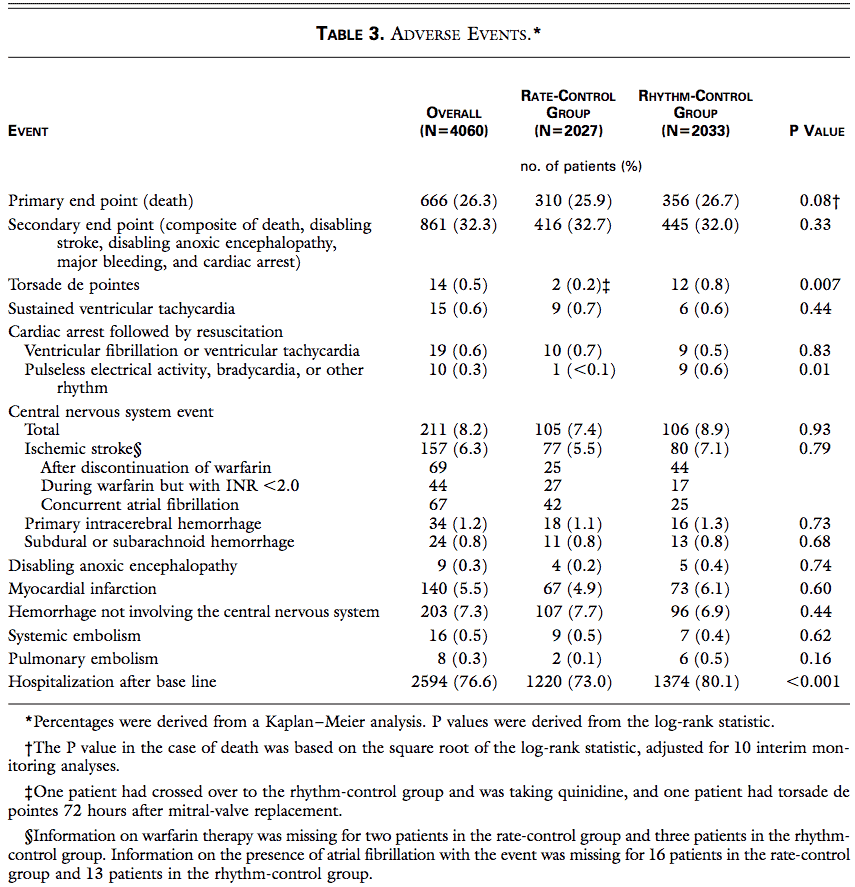
The aforementioned study analyzes many adverse events associated with rhythm and rate control in atrial fibrillation. Based on the table above, in which of the following categories is rate control most likely superior to rhythm control in terms of adverse events?
A. Myocardial infarction
B. Pulmonary embolism
C. Sustained ventricular tachycardia
D. Torsades de pointes
Answer: D
Table 3 in the study allows the reader to discern adverse events that could be associated with rate control and rhythm control and provides P values to inform the reader of the statistical significance. In many studies, a threshold of a P value ≤ 0.05 is set to reject the null hypothesis. The following adverse events had P values of 0.05 or less:
- torsades de pointes,
- pulseless electrical activity, bradycardia, or other rhythm, and
- hospitalization after baseline.
An appropriate interpretation of this table and these P values reveals there is a significant difference between the two groups and rate control is superior to rhythm control in these categories (if the threshold used is a P value of 0.05). The lower the P value, the lower the likelihood that the null hypothesis is actually true.
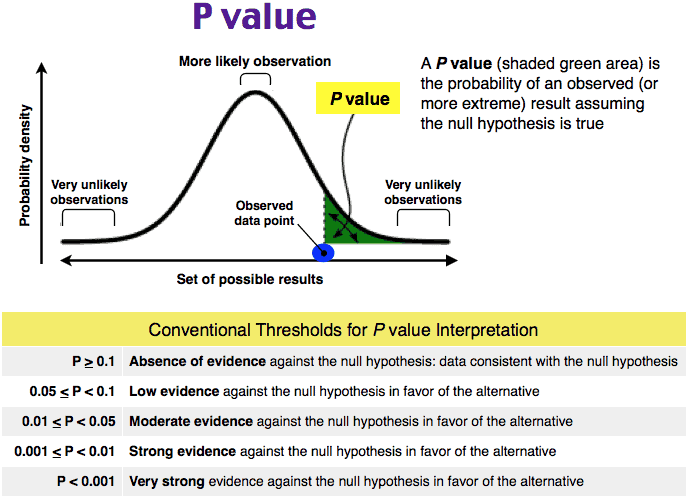
Myocardial infarction (A) has a P value of 0.60, pulmonary embolism (B) has a P value of 0.16, and sustained ventricular tachycardia (C) has a P value of 0.44, all of which suggests there is not a significant difference between the rate control and rhythm control groups for these adverse events. These larger P values mean there is a larger probability that the null hypothesis is true.
One Step Further Question: What is the treatment of choice of torsades de pointes in a hemodynamically stable patient?
Answer: Magnesium.
This is a great way to engage residents with foundational journal club knowledge, integrate evidence-based medicine into your curriculum, and utilize spaced repetition and retrieval practice to improve knowledge comprehension and retention.
Contact us if you are interested for free at your program.
Get Free Access and Join Thousands of Happy Learners

You must be logged in to post a comment.
Comments (0)