
The First Med-Peds Qbank to Help You Pass Your Internal Medicine and Pediatrics Board Exams




To prepare for your boards as a Med-Peds resident, you may feel like you have to recreate the wheel to craft your study plan. As if one board exam isn’t enough, you face the challenge of finding two great study resources to ace your exams. But the more time you spend searching for multiple board review resources, the less time you have to learn the material and feel confident on exam day. Now, with the Blueprint/Rosh Review Med-Peds Qbank, you can start learning (and stop searching) right away.
How Do You Choose a Qbank?
Previously, you might have considered the MKSAP, NEJM Knowledge+/AMBOSS, or UWorld for internal medicine. For pediatrics, you might have considered PREP, MedStudy, or BoardVitals.
Blueprint/Rosh Review’s Med-Peds Qbank gives you access to both the Internal Medicine and Pediatrics Qbanks, which you can easily toggle between with customized dashboards. This means you can access up to 5,000 questions and comprehensive explanations based on the ABP and ABIM content blueprints, so you can create your study schedule around your two board exams and seamlessly switch between specialties.
How to Study for the Internal Medicine and Pediatrics Boards with a Qbank
First things first, how should you study for your boards? With so much content to cover, we recommend targeting your “unknown unknowns.” These are concepts you don’t know (and don’t even know they exist). How do you determine them? Like this:
- Answer a question from the Qbank you’re focusing on (internal medicine or pediatrics)
- If you answer incorrectly, read the explanation
- Take notes about why the correct answer is correct, and make sure to take notes on anything in the explanation that you didn’t already know (be sure to keep your notes organized by topic)
If you do this for every question you answer incorrectly, and if you regularly review your notes and add information to topics as you do more questions, you’ll eventually determine your unknown unknowns. In return, you’ll uncover most of your blind spots that questions on the boards can ask about.
When you’re balancing studying for two board exams, set a consistent study goal (such as getting through X questions per week from the relevant Qbank, aiming to complete at least 1,000 to 2,000 questions to prepare for your exam). This can help you set aside plenty of time to determine your unknown unknowns and feel confident on exam day.
Now let’s take a look at some of the content found in the Med-Peds Qbank.
Internal Medicine
A 53-year-old man presents to his primary care physician with fatigue, erectile dysfunction, decreased libido, and arthralgias of his bilateral second and third fingers for the past 5 months. He reports no clear inciting event or trauma, sleeping problems, or mood changes. He takes no medications and does not drink alcohol or use drugs. Review of systems is negative for fever or other symptoms. On vital signs, he has a T of 98.6°F, HR of 72 bpm, BP of 118/74 mm Hg, RR of 14/min, and SpO2 of 98%. On physical exam, the patient has moderate hepatomegaly and bilateral testicular atrophy. Mild enlargement and tenderness of his bilateral second and third metacarpophalangeal joints is also present. X-ray of his hands is notable for hooklike osteophytes at his second and third metacarpophalangeal joints without erosions. Which of the following is the most likely diagnosis for this patient?
A) Hereditary hemochromatosis
B) Metabolic dysfunction-associated steatotic liver disease
C) Rheumatoid arthritis
D) Wilson disease
Answer: A
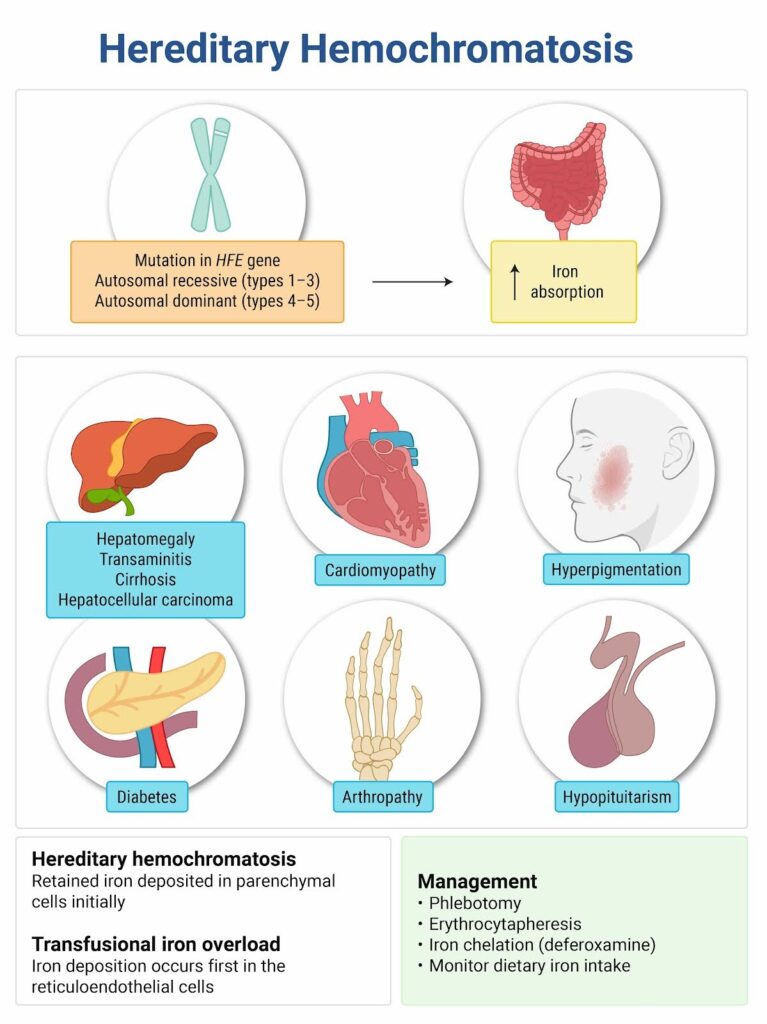
Hereditary hemochromatosis is a common genetic disorder. Affected men often present at age 40 or older, nearly 10 years earlier than affected women (due to delay in disease manifestations in women from menstrual blood). Most patients with hereditary hemochromatosis carry a mutation in their HFE gene.
The condition results in increased intestinal dietary iron absorption. Increased iron deposition causes multisystem end-organ damage such as congestive heart failure, dilated cardiomyopathy, dysrhythmia, diabetes, and cirrhosis. Other symptoms include fatigue, abdominal pain, arthralgias, impotence, decreased libido, and amenorrhea. Physical exam findings include skin bronzing, hepatosplenomegaly, and testicular atrophy. Arthralgia most commonly affects the second and third metacarpophalangeal joints. Hand radiographs can have characteristic findings of hooklike osteophytes and squared-off bone ends of affected joints as well as chondrocalcinosis. First-line evaluation includes measurement of transferrin saturation and ferritin levels. Patients with elevated transferrin saturation or ferritin levels should undergo HFE genotype testing.
Treatment for patients with hereditary hemochromatosis and iron overload typically entails iron removal, often with phlebotomy. While some complications of hereditary hemochromatosis (e.g., cardiomyopathy, glucose intolerance, skin changes) may be reversible with iron removal, other complications (e.g., arthropathy, cirrhosis) are unlikely to be reversible.
Metabolic dysfunction-associated steatotic liver disease (B) can present with fatigue, abdominal discomfort, and hepatomegaly. While a modest degree of iron overload may occur in metabolic dysfunction-associated steatotic liver disease due to increased intestinal iron absorption, hypogonadism and arthralgias are not characteristic.
Rheumatoid arthritis (C) characteristically presents with symmetric inflammatory arthralgias affecting small joints of the hands (such as the metacarpophalangeal and interphalangeal joints) as well as the wrists, shoulders, elbows, and lower limbs. Fatigue and low-grade fever may be present, but hepatomegaly would not be expected. Hand radiograph of affected joints may show osteopenia, joint space narrowing, and bony erosions.
Wilson disease (D) is a condition of impaired copper excretion marked by copper accumulation, especially in the liver, brain, and cornea. Patients with Wilson disease typically present in childhood and early adulthood with liver disease and neurologic manifestations. Arthralgias (most commonly affecting the knees) and impotence are rare complications.
One Step Further Question:
Should relatives of patients with hereditary HFE-related hemochromatosis undergo screening for hereditary hemochromatosis?
Answer: First-degree relatives should undergo screening with iron studies and HFE gene mutation analysis.
Teaching Images
Here’s a glimpse of a couple of the thousands of teaching images in the Med-Peds Qbank:
Pediatrics
A 3-year-old boy presents with fever for the past 6 days. He has been fussy with poor oral intake. He has also developed conjunctivitis, an erythematous rash over the entire body, erythema of the palms and soles, and a red tongue. What is the cause of his findings?
A) Infection transmitted by a Dermacentor tick
B) Inflammation of medium-sized arteries
C) Toxin production by group A Streptococcus
D) Vaccine-preventable viral illness
Answer: B
This child meets criteria for a diagnosis of Kawasaki disease, which is also known as mucocutaneous lymph node syndrome. Kawasaki disease results from inflammation of medium-sized arteries. The trigger for the vasculitis is unknown. Some affected children have preceding respiratory or gastrointestinal viral infections. Some children may also be genetically predisposed to the development of Kawasaki disease, and several possible associated genes have been identified. Kawasaki disease most commonly inflames the coronary arteries, but any artery may be affected. The acute phase of vasculitis is a necrotizing arteritis, and it is during this phase that patients are at the greatest risk of developing aneurysms. This phase is followed by a subacute and chronic arteritis that may cause the formation of fusiform aneurysms. In the final stage of arteritis, myofibroblasts proliferate in the artery lumen, causing arterial stenosis. The stenosis predisposes affected patients to ischemic heart disease and coronary artery thrombosis, which may result in myocardial infarction.
An early diagnosis of Kawasaki disease is important for initiating treatment and decreasing the risk of coronary artery dilation and aneurysms. A clinical diagnosis of Kawasaki disease requires at least 5 days of fever and a minimum of four out of the five clinical criteria: bilateral nonexudative conjunctivitis; mucous membrane changes such as strawberry tongue or cracked lips; rash; extremity changes such as swelling of the hands and feet, erythema of the palms and soles, or periungual peeling 2–3 weeks after disease onset; and cervical adenopathy with node > 1.5 centimeters in diameter. First-line therapy for Kawasaki disease includes a single dose of intravenous immune globulin and aspirin, initially at anti-inflammatory dosing, and then lowered to antiplatelet dosing after the child is afebrile for 48 hours.

Rocky Mountain spotted fever (RMSF) is an infection transmitted by the Dermacentor (A) species of ticks and is an important differential diagnosis for a child with fever and rash. In contrast to the palmar-plantar erythema of Kawasaki disease, the rash of RMSF is classically petechial over the wrists, ankles, palms, and soles. Patients with RMSF typically experience significant headache and myalgias. Conjunctivitis is variably present in RMSF, but a red tongue is not characteristic.
Toxins produced by group A Streptococcus (C) may cause scarlet fever or toxic shock syndrome. Scarlet fever occurs in association with streptococcal pharyngitis, but the patient has not reported sore throat and has no evidence of tonsillitis, pharyngeal exudates, or lymphadenopathy noted on examination. The rash of scarlet fever is typically diffuse and erythematous with a rough, sandpaper feel. It spares the circumoral area and the palms and soles. A diagnosis of toxic shock syndrome requires both the presence of hemodynamic instability and organ dysfunction, such as renal insufficiency or coagulopathy. Neither shock nor organ dysfunction is described in this patient.
Vaccine-preventable viral illnesses (D) such as measles cause fever and exanthem. Measles also classically includes bilateral conjunctivitis, often with lacrimation or photophobia. Measles sometimes causes an enanthem of Koplik spots, small blue-grey elevations that are often located on the buccal mucosa, but a red tongue is not an associated feature. In addition, measles would not explain the patient’s palmar-plantar erythema.
One Step Further Question: What is the risk of coronary artery aneurysms in patients with Kawasaki disease who are treated with intravenous immune globulin in a timely manner?
Answer: Less than 5 percent.
Teaching Images
Here are a couple more of the thousands of teaching images in the Med-Peds Qbank:

As you prepare for your internal medicine and pediatrics board exams, remember Blueprint/Rosh Review is by your side. The Med-Peds Qbank has a Pass Guarantee, so if you don’t pass, you get your money back or extend your subscription for another year at no cost.
Get started with the only Qbank dedicated to Med-Peds. To make sure it’s right for you, try it for free first.
We also offer Pediatric Hospital Medicine Board review from Blueprint/Rosh Review.
Get Free Access and Join Thousands of Happy Learners

You must be logged in to post a comment.
Comments (0)