A is the correct answer. Why?
Get More MyEMCert Questions
The most up-to-date questions for all current modules.
A Amniotic fluid embolism
B Eclampsia
C Postpartum cardiomyopathy
D Pulmonary thromboembolism
E Sepsis from chorioamnionitis
Explanation
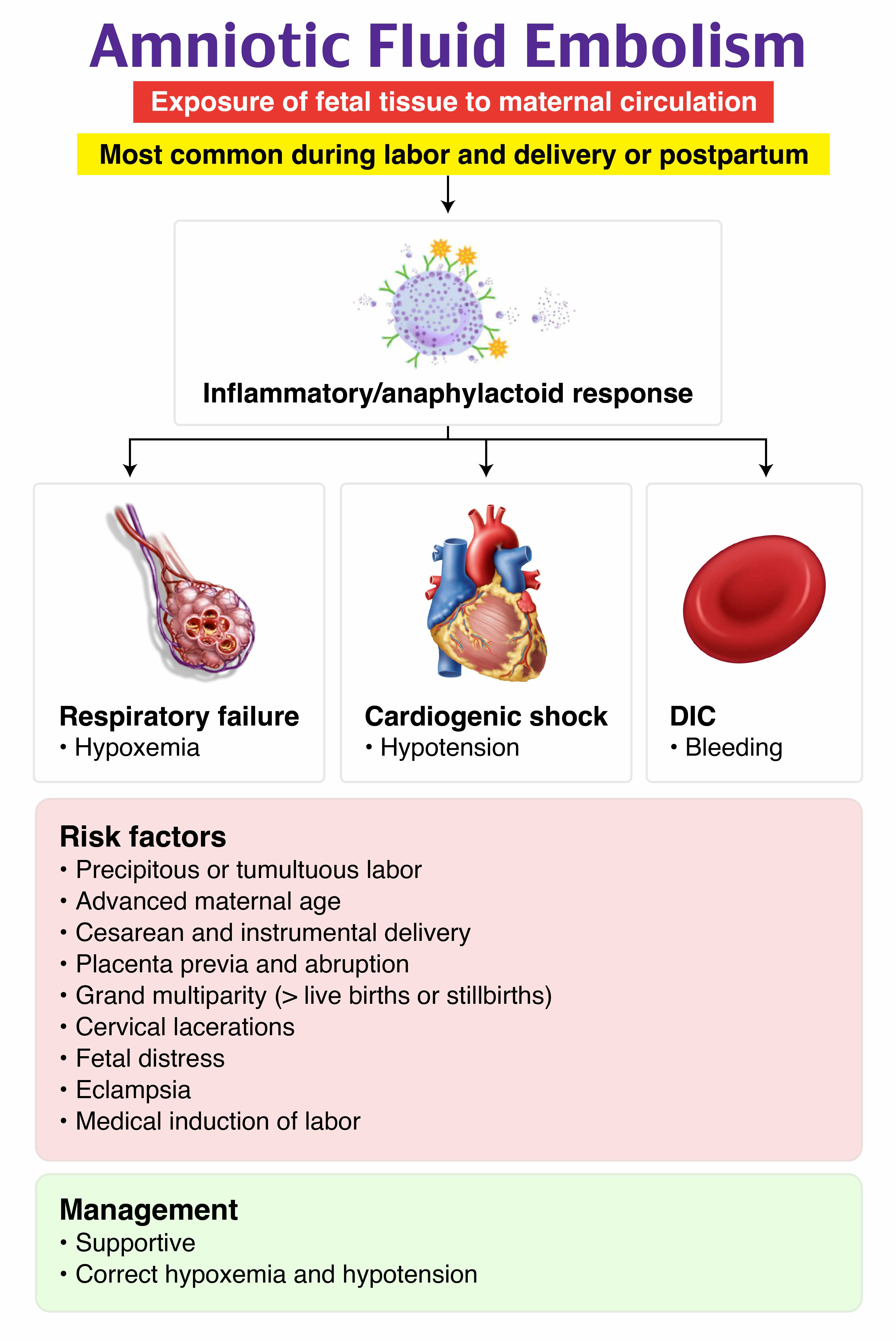
Amniotic fluid embolism (AFE) is a rare but catastrophic obstetric emergency that typically occurs during labor, delivery, or immediately postpartum. It carries a high maternal mortality rate of 20–60%. AFE results from the entry of amniotic fluid, fetal cells, hair, or other debris into the maternal circulation, triggering an abnormal immune response. This leads to pulmonary vasospasm, acute right heart failure, hypoxia, and often disseminated intravascular coagulation (DIC), which is a hallmark of the syndrome.
Risk factors include advanced maternal age, multiple gestation, cesarean or instrumental delivery, precipitous delivery, placenta previa or abruption, and induction of labor. The most common presentation involves sudden hypoxia, hypotension, and altered mental status or seizures during labor or within 30 minutes postpartum. Coagulopathy is seen in most cases. The diagnosis is clinical and remains one of exclusion, as there are no definitive laboratory or imaging findings. Chest radiography may show nonspecific findings like pulmonary edema or infiltrates. Echocardiography may demonstrate acute right heart strain but is not diagnostic.
Emergency department management focuses on aggressive supportive care: securing the airway, maintaining oxygenation, initiating fluid resuscitation, starting vasopressors for shock, and beginning transfusions for DIC. Advanced interventions may include ECMO in refractory cases. Obstetric and critical care consultation is essential.
While eclampsia (B) can present with seizures and altered mental status in a peripartum woman, it typically occurs in the context of preeclampsia, marked by hypertension and proteinuria. This patient’s hypotension and hypoxia are inconsistent with eclampsia and instead point toward cardiovascular collapse, which is classic for AFE.
Postpartum cardiomyopathy (C) usually occurs days to weeks after delivery and presents with progressive symptoms of heart failure such as dyspnea, orthopnea, and fatigue. It is not associated with seizures. The acute onset of symptoms within minutes of delivery strongly argues against postpartum cardiomyopathy and supports AFE.
Pulmonary embolism (PE) (D) is a critical differential diagnosis and may present with sudden dyspnea, hypoxia, and hypotension, similar to AFE. However, it rarely causes seizures. The abrupt onset of cardiovascular collapse in the setting of delivery favors AFE over thromboembolism. PE is more common later postpartum and generally has a more subacute presentation.
Sepsis (E) can cause hypotension and altered mental status, but it typically develops over hours to days, not minutes. Chorioamnionitis usually presents with maternal fever, uterine tenderness, and fetal tachycardia before delivery. This patient’s immediate cardiovascular collapse and seizure are not consistent with sepsis and are more characteristic of AFE.