
Announcing the New Mock Family Medicine Shelf/Clerkship Exam

Related Articles


Introducing the Mock Family Medicine Shelf/Clerkship Exam, best suited for medical students who want to excel in their family medicine clerkship.
The Mock Family Medicine Shelf/Clerkship Exam is located in your Boost Box (on the home page of your desktop/laptop Rosh Review account). It contains 100 questions and comprehensive explanations to help you prepare for the NBME Family Medicine Shelf Exam.
Categories covered include topics such as hypertension, neoplastic disease, and preventive care with a few “zebras” to keep you on your toes.
Here is an example of a question and explanation:
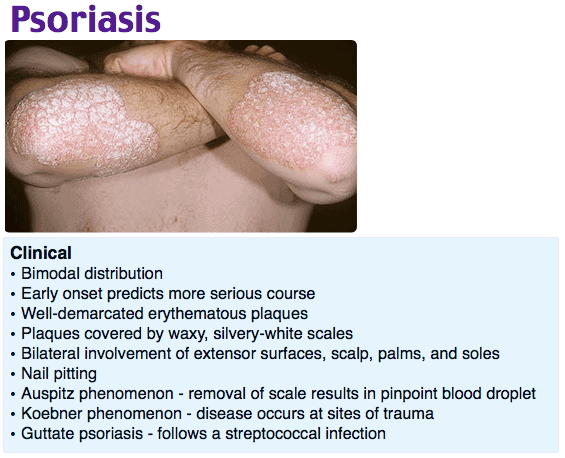
A 27-year-old woman presents with a multi-year history of large plaques on her bilateral lower extremities. She denies pruritus and a history of atopy. Examination revealed large erythematous plaques with silvery scales covering her lower extremities and trunk, sparing skinfolds, the face, oral mucosa, and acral surfaces. A potassium hydroxide preparation is negative. Which of the following is your diagnosis based on the history?
A. Nummular eczema
B. Psoriasis
C. Seborrheic dermatitis
D. Tinea corporis
Answer B
Psoriasis is a chronic inflammatory skin condition that is immune mediated. It has a hereditary predisposition with onset between 15 to 30 years of age. Risk factors include direct skin trauma (Koebner phenomenon), streptococcal throat infection, and smoking. The diagnosis is often made clinically; biopsy is rarely needed for confirmation. Typical lesions are well-defined erythematous, scaly, silvery plaques that differ in size, are pruritic, and are occasionally painful. These plaque psoriasis lesions occur on the extensor surfaces of the arms, legs, scalp, buttocks, and trunk. Atypical forms include guttate, pustular, erythrodermic, and inverse psoriasis. Other manifestations include psoriatic onychodystrophy (abnormal nail plate growth) and psoriatic arthritis, which is not related to the severity of the skin disease. Mild/moderate psoriasis affects less than 5% of the body surface area and spares the genitals, hands, feet, and face. It is treated with corticosteroids, vitamin D analogs, tazarotene intermittently, or calcineurin inhibitors continuously. Severe psoriasis involves more than 5% of the body surface area or involves the hands, feet, face, or genitals and should be referred to a dermatologist for treatment with vitamin D analogs, systemic therapy, and phototherapy. A rheumatologist can treat arthritis symptoms with tumor necrosis factor inhibitors. Patients suffering from psoriasis are at increased risk of developing depression, immune-mediated inflammatory conditions, malignancy, metabolic syndrome, and myocardial infarction. Psoriasis causes noteworthy social morbidity that negatively affects the life of the patients by causing issues with work, activities of day to day living, and socialization.
Nummular eczema (A) is usually seen in atopic patients and can be ruled out based on clinical background. Histology could provide further support to the diagnosis. Seborrheic dermatitis (C) affects the sebaceous glands and hair follicles on the scalp and face. Lesions of tinea corporis (D) are typically scaling, annular lesions with erythematous borders and central clearing. The lesions are typically pruritic. Potassium hydroxide preparation shows branching hyphae.
One Step Further question:
Which type of psoriasis occurs in skin folds such as flexor surfaces and perineal, inframammary, axillary, inguinal, and intergluteal areas?
Answer:
Inverse psoriasis.
We also have mock shelf exams available for emergency medicine, internal medicine, OB/GYN, pediatrics, and psychiatry. And be sure to check out our family medicine board review question bank for thousands of comprehensive questions.
If you’re interested in How to Crush Your Family Medicine Shelf Exam, How to Increase Your Family Medicine Certification Exam Score by 100 Points, and other tips about all things family medicine, head over to the Rosh Blog.
Study on,
The Rosh Review Team
Get Free Access and Join Thousands of Happy Learners

You must be logged in to post a comment.
Comments (0)