Urinary incontinence is a common concern as women age and can have a detrimental effect on their quality of life. Urinary incontinence can be categorized as stress, urge, or mixed incontinence. This patient has stress urinary incontinence, defined as leakage of urine with physical exertion, such as laughing, coughing, or sneezing. There are six minimum steps of evaluation for this condition: history, urinalysis, physical examination, demonstration of stress incontinence, assessment of urethral mobility, and measurement of postvoid residual volume. If the evaluation clearly points to uncomplicated stress urinary incontinence, a midurethral sling is a popular and effective surgical treatment.
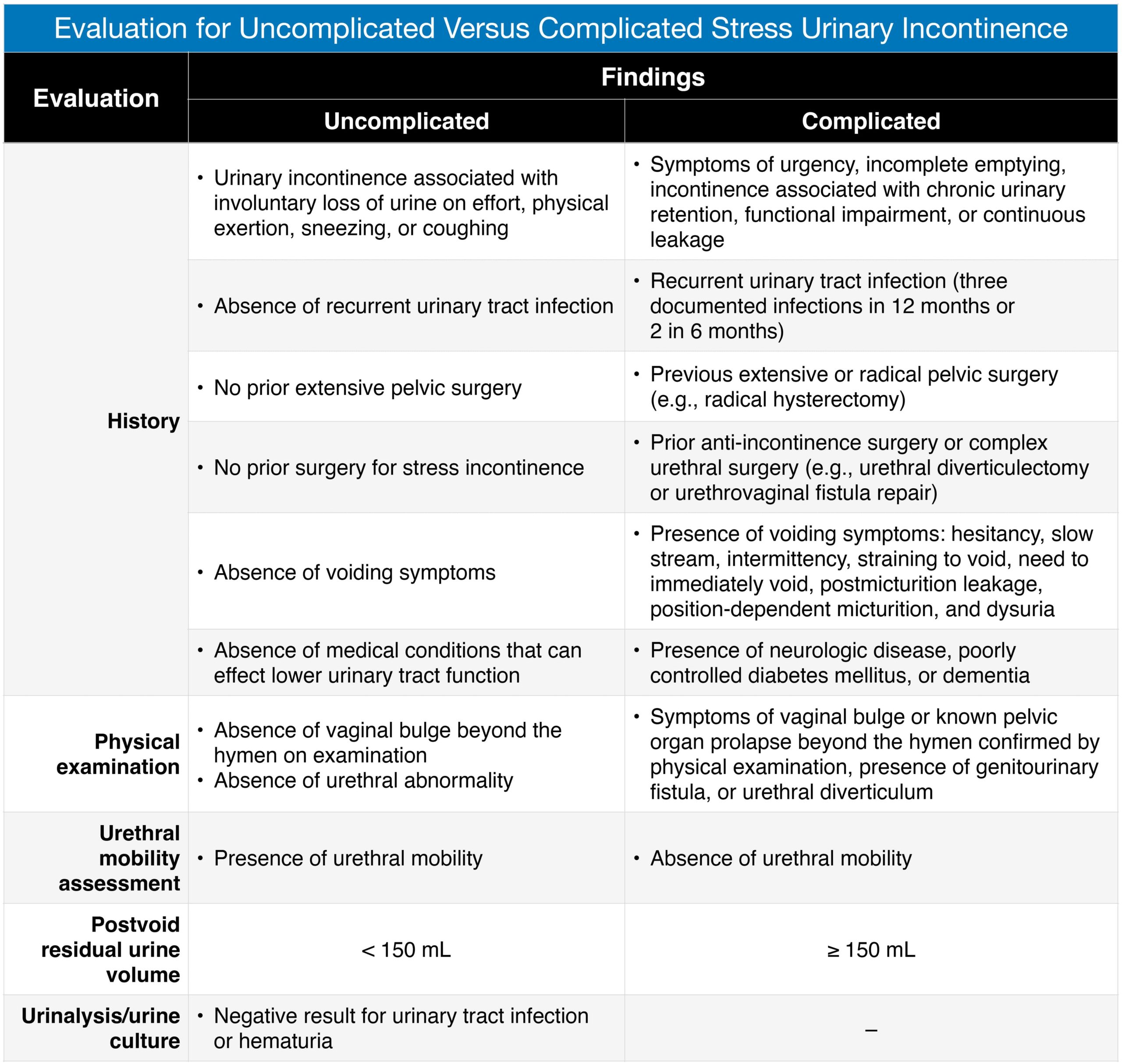
If this patient’s medical history merits blood work and an ECG (A) prior to surgical intervention, this may be appropriate, but this is not the best next step until the stress incontinence evaluation has been completed. Stress incontinence may be characterized as complicated if the patient describes symptoms of urgency, difficulty voiding, or recurrent urinary tract infections in her history; if she has had prior surgery for incontinence; if there is pelvic prolapse beyond the hymen, genitourinary fistula, or urethral diverticulum, or absence of urethral hypermobility on physical exam; or if she has an elevated postvoid residual. In cases of complicated stress urinary incontinence, multichannel urodynamic testing (B) is warranted. This patient does not have any of the above complicating factors. However, in keeping with the 6 minimum steps for evaluating her condition, an additional test is required before proceeding with surgery (C), the measurement of postvoid residual.